Patient-Centered Payment for Care of Chronic Conditions
The Importance of Effective Chronic Condition Care
The majority of adults in the United States have a chronic condition such as arthritis, asthma, chronic obstructive pulmonary disease (COPD), diabetes, heart disease, or kidney disease, and more than one-fourth have two or more chronic conditions.1 In addition, more than one-sixth of children under age 18 have a chronic health condition.2
On average, healthcare spending is six times as high for patients who have chronic conditions as for those who don’t.3 Although most of that spending pays for treatment and management of the chronic conditions, a significant portion is used for treatment of the complications that arise from inadequate care.4
In addition, undiagnosed and poorly managed chronic conditions reduce the productivity of working-age adults; for many chronic conditions, the cost of lost productivity for the workers and their employers exceeds the amount spent on healthcare services.5
Many chronic conditions can be managed effectively by a primary care practice if the practice has adequate time and staff to do so, but current payment systems do not support this. Patient-Centered Primary Care Payment is needed to give primary care practices sufficient resources and flexibility to provide appropriate, effective care for many patients with chronic conditions.6
However, some patients will need support from a specialist in addition to a primary care practice for one or more aspects of their care:
- Diagnosis. In some cases, it is difficult to determine whether a patient has a chronic disease without specialized training and experience. Many patients are misdiagnosed, particularly those with less common conditions and conditions with symptoms similar to other diseases.7 An inaccurate diagnosis can lead to unnecessary or harmful treatment for a non-existent condition and/or failure to properly treat a chronic condition that does exist. In addition, many patients receive unnecessary tests and/or unnecessarily expensive tests to rule out unlikely diagnoses.8 In some cases, these tests can lead to false positive results that contribute to inaccurate diagnoses and unnecessary treatments.
- Treatment Planning. There are generally multiple approaches to treating a diagnosed condition. In some cases, the safest and most effective treatment will depend on the exact nature of the patient’s condition and on any other health conditions the patient has and the medications they are taking for other conditions. In some cases, there are tradeoffs between effectiveness, safety, side effects, and cost among different treatment options, and patients will need information and assistance in determining which option is best for them. As new therapies are developed, and as new evidence is developed about the effectiveness and safety of different therapies, patients will need to have the most current information in order to make the best choice. Because primary care physicians treat a wide range of different conditions, it is difficult for them to stay current on treatment options and tradeoffs, particularly for less common conditions.
- Care for Severe, Complex, and Uncommon Conditions. Patients who have severe conditions, uncommon conditions, multiple chronic conditions, and patients for whom standard treatments are not effective or have problematic side effects may need specialized expertise or services that a primary care practice cannot provide. In addition, some patients whose chronic condition is being effectively managed by a primary care practice may need to temporarily receive treatment and management services from a specialist, such as when the patient experiences an acute condition that complicates management of the chronic condition until the acute condition is resolved.
Consequently, in order for all patients to receive the most effective care, it is not enough to pay adequately for primary care. Specialists who diagnose and treat chronic conditions also need to receive adequate and appropriate payments for their services.
The Problems With Current Payment Systems
Problems With Fee-for-Service Payment
Current fee-for-service payment systems make it difficult for specialists as well as primary care practices to provide all of the services needed by patients with chronic conditions:
- Inadequate time for accurate diagnosis and successful treatment planning. The amounts Medicare and health insurance plans pay for office visits are often not large enough to allow a specialist to spend the time necessary to accurately diagnose complex symptoms and to work with the patient to develop a treatment plan that is appropriate and feasible for that patient. As a result, patients can be misdiagnosed or fail to receive an accurate diagnosis in a timely fashion, and patients can receive unnecessarily expensive treatments or a treatment plan they are unable to follow.
- Lack of payment or inadequate payment for high-value services. There is often no payment at all for many of the high-value services specialty practices should deliver to help patients with chronic conditions, such as phone calls to monitor a patient’s condition in order to respond quickly when problems arise, education from nurses or other practice staff about how to successfully manage the patient’s condition, and palliative care services for a patient with an advanced illness. Even when fees for these services are available, not all patients who need them are eligible, and/or the fee amounts are lower than the cost of delivering the services appropriately. As a result, patients with severe and complex chronic conditions may have emergency department visits, hospitalizations, and hospital readmissions that could have been avoided if the physician practice had been able to deliver more proactive care.
In addition, current fee-for-service payment systems do not assure that patients will receive appropriate, high-quality services even when payments are available for those services:
- No assurance of the appropriateness or quality of the services delivered to each patient. Under fee-for-service payment, physicians and other providers are paid for delivering a service to a patient even if the service was unnecessary, and the fee is the same regardless of the quality of the service provided.
- Financial penalties for successful treatment. Specialists who treat patients with chronic conditions are typically paid based on the number of times the patient comes to the physician’s office and the number of treatments the physician practice provides. As a result, the specialty practice is penalized financially if it helps the patient avoid exacerbations or slow the progression of their condition.
Problems With Value-Based Payments
The value-based payment programs created by Medicare and most health insurance plans have done little to support higher-quality specialty care for patients with chronic conditions because they do not correct the problems in the current fee-for-service payment system. Moreover, because they focus primarily on reducing spending, not on improving the quality of care, and because they do not adjust measures of spending or quality for differences in patient needs, they can make it more difficult for the patients who most need specialty care to receive it.
Problems with Pay-for-Performance Programs
In the Medicare program and some health insurance plans, specialists who diagnose and treat chronic conditions may receive higher or lower payments based on their performance on measures of quality, utilization, and/or spending. This approach is problematic for a number of reasons.
- There are no changes in fees for services. Typical pay-for-performance systems do not provide any new or different payments for services that are not adequately supported by existing fees. The bonus payments available are generally too small to offset the loss of fee revenues that physician practices experience when patients need fewer office visits or treatments, and the bonuses may not even cover the additional administrative costs practices incur to submit data needed to document good performance. As a result, they do not enable specialists to deliver care in different ways that would result in better outcomes or lower costs.
- There are no reliable measures of quality for many types of chronic conditions. There are no measures available for many of the less common conditions treated by specialists. Even where a measure does exist, it may not provide a reliable assessment of quality when a physician only has a small number of patients with that specific condition. As a result, specialty practices are rewarded or penalized based primarily or solely on how they treat the subset of their patients who have commonly-occurring conditions.
- Quality measures for common chronic conditions are not designed for the types of patients seen by specialists. The quality and utilization measures typically used to assess performance for specialists are the same as the measures used for primary care practices. They are based on averages for all patients with the chronic condition, not the subset of patients with complex and difficult-to-manage forms of the condition whose care generally needs to be managed by specialists. These patients are more likely to require additional services and expensive treatments and less likely to achieve good outcomes. As a result, specialists can be penalized for focusing on the subset of patients with a chronic condition who most need their services or for providing customized treatment based on individual patient needs. This can make it difficult for patients with more complex conditions to obtain the care they need.9
- There is no assurance of high-quality care for individual patients. Even if there are measures of quality that are appropriate for the kinds of patients a specialist sees, the specialist will still be paid for delivering an inappropriate or low-quality service to an individual patient, regardless of how the specialist performs on the quality measures.
- The payments discourage collaborative approaches to improving care. In many pay-for-performance programs, such as Medicare’s Merit-Based Incentive Payment System (MIPS), a physician can only receive a bonus payment for good performance if other physicians have been penalized for poor performance. This discourages collaborative efforts to improve care, because if a high-performing physician practice helps other practices to improve, the high-performer could receive a smaller bonus.
Problems with Bundled/Episode Payment Programs
Two bundled payment demonstration programs have been implemented in Medicare that included patients with specific types of chronic diseases, including patients with asthma, chronic obstructive pulmonary disease (COPD), diabetes, and heart failure:
- In 2013, the Center for Medicare and Medicaid Innovation (CMMI) implemented the Bundled Payments for Care Improvement (BPCI) demonstration program.10 It was designed to reduce spending during an episode of care that started with a hospital admission and ended 90 days after discharge. If spending during an episode was lower than a “target price” established by CMMI, the physician group or hospital that delivered the patient’s hospital care was eligible to receive a bonus payment, and if spending was higher, the provider would have to pay a penalty. Although the majority of the patients in the program had hip or knee surgery or were hospitalized for a serious acute condition, there were also a large number of patients included who were hospitalized for an exacerbation of asthma, COPD, or heart failure.
- The BPCI program was replaced in 2018 with the Bundled Payments for Care Improvement – Advanced program (BPCI-A), which defines episodes similarly to BPCI, but uses a different methodology for determining bonuses and penalties.11 Although there were a number of changes in the types of patients and procedures that were eligible to participate, patients hospitalized for asthma, COPD, or heart failure continued to be eligible.
Because of the way they were designed, these bundled payment programs have done nothing to improve care for the majority of patients who have chronic conditions, and they have not solved the problems in current fee-for-service payments for the patients who are included:
- Patients are only eligible if they are hospitalized. Only a small percentage of patients with chronic conditions such as asthma, COPD, and heart failure are hospitalized during the course of the year, but these are the only patients who have been eligible to participate in BPCI and BPCI-A. One of the key goals of effective chronic condition management is to help patients avoid exacerbations that require hospitalization, but BPCI and BPCI-A only have the potential to support that goal after a hospitalization has already occurred.
- Patients can only participate for a short period of time. Even though a patient with a chronic condition needs treatment and support throughout the year, BPCI-A is focused only on care delivered during the 90 days following a hospital discharge. If the patient is hospitalized after 90 days for a problem that could have been prevented by high-quality care, there is no penalty for the physician or hospital that was managing the patient’s care.
- There are no payments to support new or improved services. Although these are described as “bundled” payment programs, the participating providers do not actually receive a single, bundled payment that gives them the flexibility to deliver different types of services to the patients. Each provider is still paid individually for each service, they are paid only for the services that are covered under the standard fee-for-service payment system, and they are paid the usual amounts for each of those services.
- Bonus payments may not offset additional costs or losses incurred by providers. The hospital or physician group participating in the program can receive an additional payment if Medicare determines that a minimum amount of savings has been achieved in the eligible episodes, but the only way to generate savings is to reduce the number of fee-based services the patient receives during the hospitalization or the 90-day period following discharge. Even if there are sufficient savings to qualify for a bonus payment, Medicare will not release that bonus until many months after any services were delivered. The amount of the bonus is proportional to the savings for Medicare, so it may not be sufficient to cover the costs of new services the providers delivered to the patients or to offset any losses they incurred as a result of delivering fewer fee-based services.
- There is no assurance that patients will receive high-quality care. Hospitals, physicians, and post-acute care providers that deliver services to a patient during the episode are paid for those services regardless of the quality of the individual services or the overall outcomes of the care during the episode. If a provider’s average performance on a group of quality measures is poor for all of the patients, the provider will receive a smaller bonus payment when spending decreases (or pay a larger penalty if spending has increased), but the provider will still be paid the same amount for an individual service no matter how poor the quality of that service was.
- Providers can be rewarded for withholding needed care. If patients receive fewer services than they need, the reduction in spending would be considered “savings” and the provider could receive a bonus payment. The reduction in services may not affect outcomes until after the episode ends, and even if the reduction in services does have a negative effect on quality measures, the provider could still receive a bonus payment.
- The physicians who are providing ongoing care for the patients’ chronic condition may not receive any additional resources. If there are savings sufficient to qualify for a bonus payment, that bonus will go to the hospital or the physician group that has taken financial responsibility for the hospital episodes. The physicians who care for the patients in the community may be different from the physicians who care for the patients in the hospital, and there is no requirement that a portion of any bonus payment goes to the community physicians, even if they provided additional services after the patient’s discharge that helped produce the savings (e.g., by helping patients avoid hospital readmissions or expensive post-acute care).
Problems with Accountable Care Organizations and Population-Based Payments
Aside from pay-for-performance programs, the only value-based payment program that has been available to many specialty care providers has been joining an Accountable Care Organization (ACO).
An ACO is an organizational structure, not a payment system. As ACOs were originally conceived, they were expected to involve all of the physicians, including both primary care physicians and specialists, who were providing all or most of the services for a group of patients. By forming an ACO, it was believed that the physicians would have greater ability to coordinate their services and deliver patient care more efficiently and effectively.
Although it is very desirable for patients to receive more coordinated care, it does little good to coordinate the services delivered by multiple providers if the individual providers cannot deliver high-quality care because of barriers in the payment system.12 Consequently, an ACO will have only limited benefit for patients if it is not accompanied by a better approach to paying individual physicians and other providers for their services.
Two basic approaches have been used (or proposed) for paying ACOs: (1) shared savings and shared risk, and (2) “population-based payment” (global capitation). Neither of these approaches directly solves the problems in current fee-for-service payments and both can result in lower-quality care for higher-need patients.
Problems with Shared Savings and Shared Risk
Under the shared savings and shared risk approaches to payment:
- There are no payments to support new or improved services. Providers are still paid only for the services that are covered under the standard fee-for-service payment system and they are paid the usual amounts for each of those services. If Medicare or a health insurance plan determines that the total spending on the patients who are assigned or attributed to the ACO is lower than the payer projects spending would have been in the absence of the ACO, the ACO can receive a bonus payment based on a fraction of the estimated savings. If there is also “downside risk,” the ACO has to pay a penalty if spending is higher than expected.
- Specialty care providers may not receive shared savings even if they reduce spending on their patients. If a specialist changes the delivery of care for their patients in a way that reduces total spending on those patients, that amount of savings alone will generally not be sufficient for the ACO to receive a shared savings payment unless other providers in the ACO have also been able to produce savings. Even if the ACO has produced enough savings in total to qualify for a shared savings payment, there is no assurance that any portion of that payment will go to the specialists who helped produce the savings, or that the amount they receive will cover any costs or offset any losses they incurred.
- The ACO providers can be rewarded for withholding services that patients need. Under a shared savings payment model, if a physician in an ACO does not order a test, procedure, or medication for a patient, or if a primary care physician does not refer a patient to a specialist for evaluation, that is considered “savings” regardless of whether the patient needed the service or not. The small number of simple quality measures used in shared savings and shared risk models do nothing to protect against most potential types of undertreatment.
- The ACO providers can be rewarded for overdiagnosis. “Savings” are calculated by comparing actual spending to an expected level of spending, and the expected level is calculated based on the risk scores assigned to the patients. As a result, the ACO is more likely to achieve savings if the risk scores assigned to its patients are higher. Since the risk scores are based on how many chronic conditions the patients have been diagnosed with, regardless of how effectively the ACO providers treat those diseases, the ACO is rewarded financially when it assigns additional chronic disease diagnoses to a patient. Conversely, the ACO could be penalized if a patient sees a specialist who determines they do not have a chronic condition, because the payments for the specialist’s services will increase total spending and the absence of the chronic condition diagnosis will reduce the level of expected spending.
- The ACO providers can be penalized for providing services to higher-need patients. Patients who have more severe chronic conditions and/or characteristics that require customized treatments will generally need more services and more expensive services, and the risk adjustment systems used in shared savings models do not accurately estimate how much higher spending will be for these patients. As a result, although an ACO with more high-need patients will have higher actual spending, its expected spending level may not increase by the same amount, and this will reduce the likelihood of receiving a shared savings bonus and increase the chances that the ACO will be financially penalized.
Problems with Population-Based Payment and Global Capitation
An alternative approach to paying an ACO is what is called either “population-based payment” or “global capitation.” Under this system, the ACO receives a fixed amount of money each month for each patient who is assigned to the ACO, and the ACO is then responsible for delivering or paying for all of the services the patient needs, using only the revenues from those monthly payments. Some large physician practices, independent practice associations, and health systems are paid this way by HMO insurance plans, and CMS has created a demonstration program called “Global and Professional Direct Contracting” (GPDC) in which entities similar to ACOs called Direct Contracting Entities (DCEs) can receive capitation payments instead of fees for some or all of the services delivered by the providers in the DCE.13 Under this approach:
- Specialty care providers generally still receive only standard fee-for-service payments. Although the capitation payment theoretically gives the ACO or DCE the flexibility to pay the physicians, hospitals, and other providers in different ways, in most capitated arrangements the specialists continue to receive standard fee-for-service payments because no alternative approach to paying for their specific services has been developed.
- Patients can receive less care than they need. The ACO/DCE receives a capitation payment for a patient assigned to the ACO/DCE regardless of whether that patient receives the services they need. Capitation payments are the same regardless of how many services are delivered or what types of services are delivered, but the ACO/DCE incurs higher costs when patients receive more services. As a result, even if the total payments are sufficient to support all of the services needed by the patients assigned to the ACO/DCE, the ACO/DCE will make higher profits if fewer services are delivered. The small number of simple quality measures used in population-based payment models do nothing to protect against most potential types of undertreatment.
- The ACO/DCE providers can be penalized for accepting higher-need patients. In traditional capitation systems, the payment for each patient was the same regardless of their needs. In most population-based payments, the capitation payments are “risk-adjusted” so the amounts are higher for patients with chronic conditions. However, the risk adjustment systems that are typically used do not adjust payments for the severity of the patients’ chronic conditions, for patients who develop new chronic conditions or acute conditions, or for non-medical characteristics of the patients. As a result, the ACO/DCE can be penalized if it agrees to deliver care to many types of higher-need patients.
Patient-Centered Payment for Care of Chronic Conditions
Goals of Patient-Centered Payment
A method of paying for care of chronic conditions is needed that will solve the problems of current payment systems without reducing access to care for the patients who have greater needs. In a patient-centered payment system for care of chronic conditions:
- A patient with a chronic condition should be able to receive the services that will best address their specific needs. In order for patients to receive the highest-value care, the many gaps in payment under current payment systems have to be filled.
- A patient with a chronic condition should be assured of receiving appropriate, evidence-based care. In order to be paid for diagnosis, treatment, or care management of a chronic condition, the physician practice or other healthcare provider should deliver evidence-based care to the patient unless there is no relevant evidence to guide care decisions or there are good reasons to deviate from what evidence-based guidelines recommend.
- The payment amounts should be adequate to cover the cost of delivering services in a high-quality manner to patients with chronic conditions. The payment amounts should be based on what it costs to deliver high-quality care, not based on the fees paid in the past, the amount of savings that has been produced, or an arbitrary percentage of total spending.
- A patient with a chronic condition should be able to select which physician practice or provider will deliver care for the condition based on the quality and cost of the services they will receive. There should not be any barriers, such as high cost-sharing amounts, prior authorization requirements, or narrow networks, that prevent patients from receiving the most appropriate services from the physicians and other providers best able to help them.
The Phases of Chronic Condition Care
Although every chronic condition is different, the care patients need for most chronic conditions can be divided into four distinct phases, each of which has a significant impact on the outcomes patients experience and the cost of the care they receive:
- Diagnosis. The first phase is determining whether the patient has a chronic condition and which specific condition they have. Different health problems have similar symptoms, and there is not always a diagnostic test that can definitively determine whether a patient has a specific chronic condition. In some cases, initial treatment may need to begin before a diagnosis is finalized because a definitive diagnosis can only be determined based on the effectiveness of treatment. Adequate time and sufficient expertise are required to collect the information about the patient needed for accurate diagnosis, while avoiding unnecessary testing and misdiagnosis.
- Care Planning. If a patient is diagnosed with a particular condition, there are typically multiple approaches to treating and managing the condition. The effectiveness and side effects of treatments can differ for different patients, and patients differ both in their preferences about the trade-off between effectiveness and side effects and in their ability to afford and utilize specific approaches to treatment. Patients with more advanced conditions will need palliative care services in addition to or instead of treatment. The choices and the tradeoffs will evolve continuously as new therapies are created and as new evidence emerges about the relative effects of treatments. The physician and other staff on the patient’s care team need adequate time to identify the best alternatives based on the most current evidence, and they need adequate time to educate the patient about the choices and assist them in deciding which to pursue. Adequate time and expertise in this phase are needed to avoid ineffective, harmful, and unnecessarily expensive services for the patient.
- Initial Treatment. When treatment first begins, patients will need adequate education and support to enable them to understand and follow the care plan correctly. Some patients may experience unexpected side effects or challenges in using the treatments, or the treatments may not work as well as expected, and adjustments or changes to treatment will be needed to address these problems. Failure to proactively address these issues can cause avoidable complications for the patient or prompt an unnecessary change to a more expensive or dangerous form of treatment.
- Continued Care for the Condition. Once the most effective treatment approach is determined, the patient’s condition needs to be proactively monitored so that additional assistance can be provided or adjustments to treatment can be made when needed. In some cases, the most effective treatment available will only be partially effective in controlling the patient’s symptoms, and these patients will need more intensive monitoring and additional assistance in preventing and managing exacerbations of their condition. Failure to do this can result in avoidable complications and worse outcomes for the patient.
FIGURE 1
Phases of Chronic Condition Care
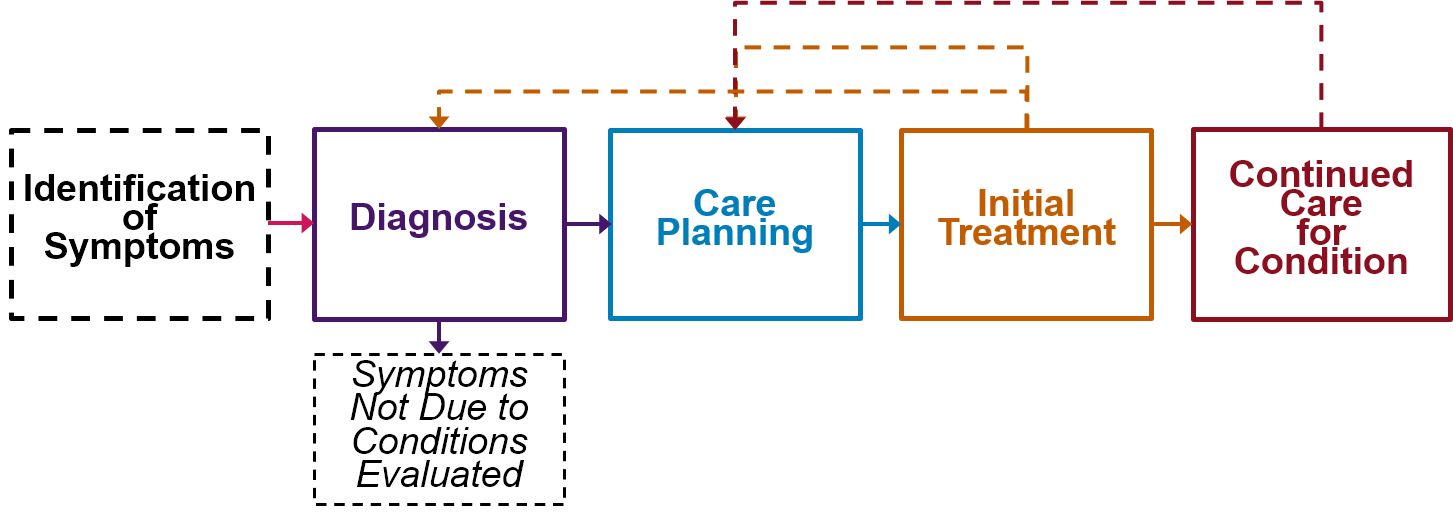
Patients may need to repeat one or more of these phases if their condition progresses, if their individual needs change, if new therapies are developed, or if new evidence emerges about the relative effectiveness of different approaches to treatment.
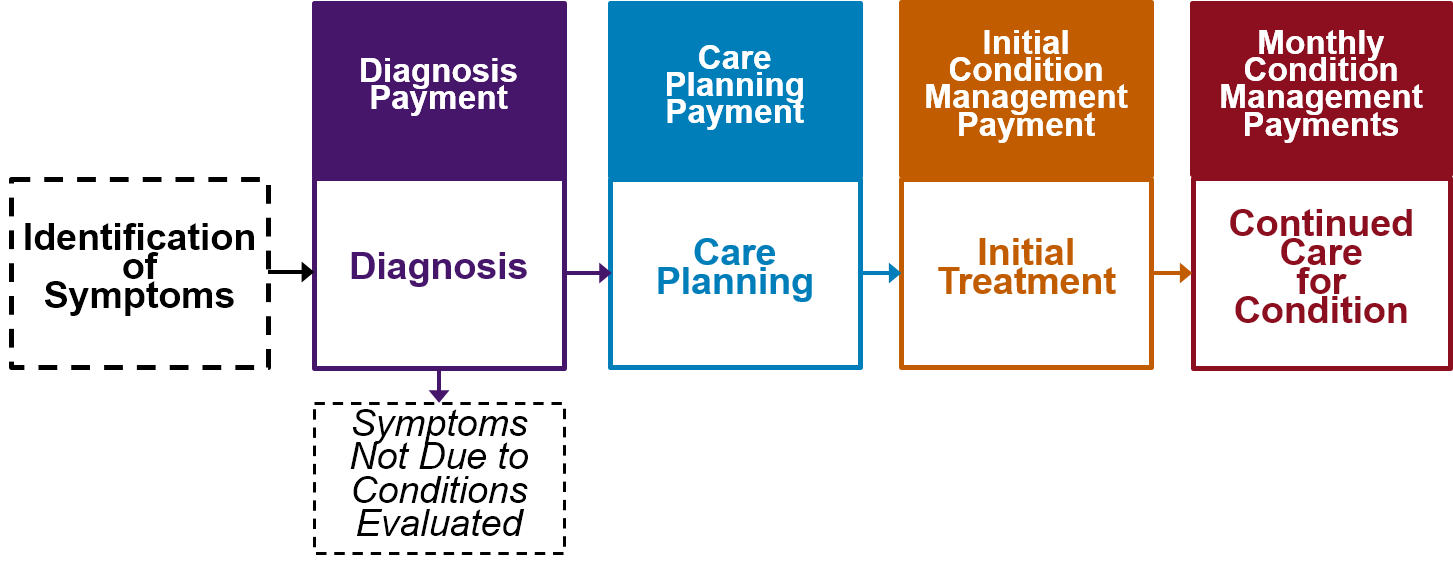
Some patients will be able to receive adequate services in each phase from their primary care practice. Other patients will need services from a specialist in one, some, or all of the phases.14 The only way to ensure that each patient can get appropriate specialty services for their specific needs, and the only way to ensure that each specialist is paid appropriately for the services they provide, is to create separate payments specifically designed to support each phase of care.
FIGURE 2
Patient-Centered Payment for Care of Chronic Conditions
Payment for Diagnosis
Method of Payment
Problems with the Current Approach
There are thousands of different billing codes and associated fees that are used to pay physicians for performing specific procedures and tests. However, there are no billing codes or fees specifically designed to pay a physician to determine the cause of a patient’s symptoms or to determine whether a patient has a specific chronic disease. In most cases, the work involved in determining a diagnosis is paid for using a generic set of fees for “Evaluation and Management Services (E/M)” that are triggered by a visit between the patient and the physician.
Because the same E/M codes and fees are used to pay for visits with physicians for many different reasons, including visits for treatment planning and monitoring of already-diagnosed symptoms as well as for diagnosis of new symptoms, there is no assurance that a payment to a specialist for one of these codes will result in a determination as to whether a patient has a particular disease or not. There is also no limit on the number of visits for which the physician could be paid before that determination is made. In contrast, for procedures and tests, the physician can only bill and be paid if the procedure or test is actually performed, and there is only one payment for an individual procedure or test.
The E/M payment will be higher if the “medical decision-making” involved is more complex or if the physician spends more time on the patient’s case, including time spent outside of the face-to-face visit with the patient. However, the same amount is paid regardless of whether extra time is needed because of the complexity of the patient’s symptoms or because the physician lacks expertise in making the diagnosis:
- A specialist with extensive experience in diagnosing a particular type of condition may be able to determine very quickly whether a patient does or does not have that condition. However, the reason the specialist does not have to spend a large amount of time diagnosing the patient may be due to the extensive time the specialist has previously spent outside of patient visits developing and maintaining the necessary expertise. In these cases, paying solely based on the amount of time the physician spends with each individual patient would not provide adequate support for the physician’s work, or it would force the physician to spend more time with a patient than is really needed merely to justify an adequate payment.15
- Conversely, a physician with little or no experience in diagnosing a condition, particularly an uncommon condition, may have to spend a considerable amount of time on an individual patient’s case, both during the patient’s visit and before and/or after the visit, in order to make a diagnosis. Moreover, if that physician orders unnecessary tests because of uncertainty about how to evaluate the patient’s symptoms, the cost to the patient and payer will be higher than necessary.
A Patient-Centered Approach to Diagnosis Payment
In a patient-centered approach to payment, a physician should receive a Diagnosis Payment that is specifically designed to support an accurate evaluation of the patient’s symptoms, regardless of how many visits the patient made with the physician.
Ideally, the Diagnosis Payment would be contingent on the specialist determining the cause of the patient’s symptoms. However, that is not always possible:
- Some symptoms can be caused by two very different types of diseases or conditions, and one specialist who sees the patient may only have the tools or expertise to evaluate a subset of those potential causes. Determining that a patient does not have one of those possible diseases is a high-value service, since it enables the patient to avoid receiving an unnecessary and potentially harmful treatment for the wrong disease, even though there may not yet be a determination of what the cause actually is or what treatment is needed. Knowing that a specific condition is not present can also reduce anxiety for the patient and avoid the need for actions such as a quarantine.
- In some cases, there may not be enough information available even for the most expert physician to accurately determine whether a patient has a particular condition or not. For example, if a patient is not currently experiencing the symptoms that prompted the evaluation, it may only be feasible to diagnose the cause when the symptoms recur. For some conditions, there are no tests available to verify the presence of the condition, or the tests are dangerous or prohibitively expensive, and the only feasible way to verify a diagnosis is to see if the treatment is effective.
Consequently, a Diagnosis Payment should be paid as long as the physician makes one of the following three determinations:
- The patient has a specific chronic condition that is causing all or part of the patient’s symptoms.
- The patient does not have any of the chronic conditions evaluated. If there is a group of chronic conditions that produce the kinds of symptoms the patient is experiencing and the physician has expertise in evaluating those conditions, the determination should include an assessment of all of those conditions, not just one. Determining that a patient does not have the conditions evaluated does not mean that the patient has no disease or other health problem at all, so an evaluation by a different specialist may also be necessary to determine a diagnosis.
- A determination cannot be made at the current time as to whether the patient has a particular chronic condition or not. If it is not possible to make a determination at the current time about the presence or absence of one or more conditions, the physician would document this and also specify what additional actions or information are needed to make a definitive determination.
The physician would only bill for a Diagnosis Payment when one of these diagnostic determinations has been completed and documented for a patient. If a patient with the symptoms being evaluated typically requires two or more visits to determine whether or not they have the condition (e.g., to order one or more diagnostic tests and then evaluate the results), there would be one Diagnosis Payment that reflects the total expected time for those visits, instead of separate fees paid for each visit. Similarly, if the determination can be made appropriately through a telehealth visit or solely through evaluation of test results without a physical examination, the Diagnosis Payment should be paid even if there was no in-person visit with the patient.
Stratifying Payments Based on Patient Complexity
If a patient has a combination of symptoms and other characteristics that require more time to evaluate correctly, the amount of the Diagnosis Payment will have to be higher so the physician making the diagnostic determination can allocate adequate time. However, the justification for higher payment should be that the complexity of the symptoms and the patient’s other characteristics requires that more time be spent in order to make an accurate diagnosis, not simply that the individual making the diagnosis takes longer to do so or decides to see the patient multiple times. This ensures that specialists are not penalized financially for evaluating more complex patients, and that specialists are not penalized for diagnosing complex patients quickly when they have the expertise and experience to do so.
The level of complexity in establishing a diagnosis is already being determined by physicians as part of the process of assigning an Evaluation and Management Services (E/M) code to a patient visit. One of four different E/M code levels is assigned to a visit with a new patient based on either (1) the amount of time spent or (2) the “level of medical decision-making” involved in the visit. Three criteria are used to determine the level of medical decision-making in establishing a diagnosis:
- the number of possible diagnoses that must be considered;
- the amount and/or complexity of medical records, diagnostic tests, and/or other information that must be obtained, reviewed, and analyzed; and
- the risk of significant complications, morbidity, and/or mortality, as well as comorbidities, associated with the patient’s presenting problem(s) and the diagnostic procedure(s).
The four different levels of payment are chosen based on the highest magnitudes assigned to two of these three criteria, as shown in Figure 3.16
FIGURE 3
Classification of Medical Decision-Making Complexity
for Current Evaluation and Management Services Payments
| Level of Medical Decision-Making | Two of the Following Three Criteria: | ||
|---|---|---|---|
| Number of Potential Diagnoses | Amount and/or Complexity of Data Reviewed | Comorbidities and Complications | |
| Straightforward | Minimal | Minimal or None | Minimal |
| Low Complexity | Limited | Limited | Low |
| Moderate Complexity | Multiple | Moderate | Moderate |
| High Complexity | Extensive | Extensive | High |
These same categories of complexity can be used to stratify the Diagnosis Payments. Since it seems unlikely that patients in the straightforward decision-making category would require evaluation by a specialist, the three higher categories of complexity (low, moderate, and high) could be used to define three levels of Diagnosis Payment:
- Low Complexity Diagnosis Payment
- Moderate Complexity Diagnosis Payment
- High Complexity Diagnosis Payment
In the current fee-for-service system, each physician assigns a level of complexity to each patient visit after the visit is made. However, from the patient’s and payer’s perspective, the Diagnosis Payments would neither be predictable nor comparable if two specialists can assign different levels of complexity and charge two different amounts for two patients with the same symptoms and comorbidities, or if the same physician could charge two different amounts for two similar patients even though the amount of work should be same.
In order to establish predictable and comparable payments, each medical specialty society could define the combinations of symptoms and other patient characteristics (e.g., age, comorbidities, and social challenges) typically seen by physicians in that specialty that would make a patient appropriate for each of the three complexity categories. This should be feasible for many chronic diseases, particularly the common chronic diseases. When a physician diagnoses an individual patient, they would assign that patient to the appropriate Diagnosis Payment Level based on their symptoms and other characteristics. Not only would this make the payment amounts more predictable and consistent for patients, it would also be less burdensome for the physician than evaluating every patient based on the three generic criteria for complexity and documenting the results. For a patient with unique symptoms and other characteristics that were not included in the standard definitions, the physician could use the general complexity criteria to assign the patient to an appropriate category and document the reasons for doing so.
As part of this process, a minimum standard could also be established for the types or combinations of symptoms that would potentially indicate the presence of one of the diseases or health problems that a particular specialist normally evaluates. If a patient does not have these symptoms, then it would be a waste of the specialist’s and patient’s time to evaluate the patient for those diseases and it would be a waste of the patient’s and payer’s money to pay for that evaluation, so the Diagnosis Payment should only be paid for patients who have those symptoms.
Payment for Assistance to Primary Care Physicians
It does not make sense for a primary care practice to refer a patient to a specialist if the patient does not have symptoms that could result from a disease or health condition in that specialist’s area of expertise. It also does not make sense to refer patients whose symptoms could be easily and accurately diagnosed by the primary care physician. Seeing these patients is not only a poor use of the specialist’s time, but it makes it more difficult for complex patients who do need to see the specialist to get an appointment in a timely fashion.
Many of these unnecessary and inappropriate referrals occur today because primary care practices are not paid adequately to enable them to spend the time necessary to determine a diagnosis or to determine which specialist(s) should see the patient. The appropriate solution to this is to implement a Patient-Centered Primary Care Payment system that pays the primary care practice adequately to make these determinations.17
However, in some cases, unnecessary or inappropriate referrals are made because the primary care physician does not have adequate knowledge or confidence to make the diagnosis themself or to determine whether the symptoms are appropriate for a referral.18 In these cases, the primary care physician needs education or assistance from a specialist about how to evaluate certain kinds of symptoms in order to either determine the diagnosis or to determine that a referral to the specialist is needed. Providing this assistance to the primary care physician requires some of the specialist’s time, but not as much time as the specialist would need to fully evaluate and diagnose the patient themself, even for a low complexity patient.
To address this, a Diagnostic Assistance Payment should be created to enable the specialist to provide support to primary care physicians in making diagnoses and referrals.19 If the patient is ultimately referred to the same specialist or specialty practice for a diagnostic evaluation, the specialist would bill for and receive a regular Diagnosis Payment instead of the Diagnostic Assistance Payment.
Billing and Payment for Diagnosis Services
This approach to paying for diagnosis services can be easily operationalized for patients who have insurance by creating four new billing codes. As shown in Figure 4, each of the four categories of services would be assigned either a CPT® (Current Procedural Terminology) code by the American Medical Association’s CPT Editorial Panel or a HCPCS (Healthcare Common Procedure Coding System) Level II code by the Centers for Medicare and Medicaid Services (CMS) HCPCS Workgroup.
FIGURE 4
Payments for Specialty Diagnosis Services
| CPT/HCPCS Code | Payment Category | Service |
|---|---|---|
| XX040 | Diagnostic Assistance Payment | Assistance to primary care in making diagnosis or determining need for referral |
| XX041 | Low Complexity Diagnosis Payment | Diagnosis of symptoms requiring low-complexity decision-making |
| XX042 | Moderate Complexity Diagnosis Payment | Diagnosis of symptoms requiring moderate-complexity decision-making |
| XX043 | High Complexity Diagnosis Payment | Diagnosis of symptoms requiring high-complexity decision-making |
The physician who is making the diagnosis would choose the appropriate CPT/HCPCS code based on the complexity category that matched the patient’s symptoms and other characteristics.
If a physician practice bills for one of these codes for a patient, the practice would not bill or be paid for an Evaluation and Management Services (E/M) payment for any visits that patient made as part of the diagnosis process.
Payment for Diagnostic Testing
The Diagnosis Payment would support the physician’s time in determining the diagnosis. The physician may also need the results of laboratory tests or imaging studies in order to make the diagnostic determination, and if so, separate payments will need to be made to the laboratory or imaging center that performs those tests. If the practice performs these tests or imaging studies itself, it should be paid separately for them.20
Accountability for Quality and Utilization
Tradeoffs in Achieving High-Quality Diagnosis
Patients and payers will want to know that the physician receiving the Diagnosis Payment has carried out the diagnosis process in a high-quality manner. In the context of diagnosis, quality has at least two key components:
- Accuracy of diagnosis. Currently, many patients are incorrectly diagnosed as having a chronic disease that they do not have, or as not having a disease that they do have. Both overdiagnosis and underdiagnosis can be harmful to the patient.
- Avoiding unnecessary or harmful diagnosis testing. Some types of diagnostic tests involve a risk of harm to the patient, such as radiation exposure during imaging or an injury or infection caused by an invasive procedure.
There are few, if any, situations, in which 100% accuracy in diagnosis is feasible. For some chronic conditions, there is no single test or even combination of tests available that can clearly indicate whether the condition is present or absent. Moreover, even where a test exists, it will have a non-zero false positive rate and a non-zero false negative rate. Because of this, there may also be no way to independently verify whether the diagnostic determination made by a particular physician is accurate.
In some cases, the most accurate diagnosis can only be determined through a test that has significant risks for the patient (e.g., an invasive procedure), or is very expensive, or both. In these cases, a tradeoff has to be made between the risks and costs of additional testing versus the risks of overtreatment or undertreatment. For example:
- The “gold standard” test for ischemic heart disease is a cardiac catheterization and angiogram, but that procedure is not only expensive, it involves a risk of injury and death for the patient. As a result, many patients appropriately receive a diagnosis of mild heart disease or no heart disease based on less definitive tests.
- A variety of genetic and biomarker tests have been developed that can be helpful in distinguishing among different potential causes of a patient’s symptoms, but many of these tests are expensive and some may only provide new or actionable information in a small number of cases.
An Evidence-Based Approach to Diagnosis Quality
The best way for physicians to achieve the most accurate diagnosis while balancing the risks and costs associated with diagnostic testing is to utilize evidence-based Clinical Practice Guidelines (CPGs) for testing and diagnosis. A Clinical Practice Guideline assembles all of the available evidence regarding how to diagnose symptoms, with consideration for the tradeoffs between accuracy, safety, and cost.21
Evidence-based Clinical Practice Guidelines exist for diagnosis of most common chronic diseases and symptoms and also for many less-common conditions. For example:
- Asthma: The National Asthma Education and Prevention Program Coordinating Committee has developed guidelines for the diagnosis of asthma.22
- COPD: The Global Initiative for Chronic Obstructive Lung Disease (GOLD) publishes guidelines for the diagnosis of chronic obstructive pulmonary disease (COPD).23
- Diabetes: The American Diabetes Association has developed a detailed Standard of Medical Care in Diabetes24, and the American Association of Clinical Endocrinologists and American College of Endocrinology have jointly developed a Comprehensive Type 2 Diabetes Management Algorithm25, each of which include guidelines for diagnosis of diabetes.
- Heart Failure: The American College of Cardiology, American Heart Association, and Heart Failure Society of America have developed a Guideline for the Management of Heart Failure which includes guidelines for diagnosis of heart failure.26
- Ischemic Heart Disease: The American College of Cardiology, American College of Physicians, American Heart Association, American Association for Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons have jointly developed a set of guidelines for diagnosis of patients with stable ischemic heart disease.27
These and other guidelines have been developed by medical specialty societies and multi-stakeholder collaboratives in order to improve both the accuracy of diagnosis and the effectiveness of treatment while avoiding the delivery of unnecessary services. The guidelines have been developed by groups of physicians, not by payers or manufacturers of specific drugs or tests, and strong efforts are made to ensure that the guidelines are based on what is best for patients.
Since Clinical Practice Guidelines define which diagnostic tests are appropriate and inappropriate in various situations, they can reduce use of unnecessary testing in a more patient-centered way than the burdensome and problematic prior authorization processes typically used by health insurance plans. For example, the guidelines for ischemic heart disease are specifically designed to avoid unnecessary use of cardiac stress testing, cardiac imaging, and cardiac catheterization, while also avoiding undertesting patients in a way that could lead to preventable heart attacks or death. In contrast, in a prior authorization process, an employee of a health insurance plan makes decisions about appropriateness of cardiac tests even though that individual has not actually examined the patient or talked with them about the many different aspects of their symptoms and history that are required to make good clinical decisions, and the health plan employee may not have any specialized expertise in the symptoms or diseases being evaluated. Use of the guidelines can also help protect physicians against malpractice lawsuits if it turns out that a diagnosis was missed that could potentially have been identified with more extensive testing.
In order to reduce variation when there are multiple diagnostic choices and the available evidence does not indicate which option is better, a recommended option can be added to the guidelines. The term “Clinical Pathway” is often used to describe a set of guidelines that recommend the use of a specific approach when the evidence is unclear or where multiple options have equivalent benefits but different costs.28
CPGs and Pathways must be developed and refined by clinicians, not by health plans. Clinicians will be more likely to utilize and adhere to clinician-developed guidelines than rules or pathways developed by payers or other entities where cost considerations may have taken precedence over patient outcomes in defining recommendations.29 In addition, a CPG developed by clinicians can be used for all patients, regardless of payer.
Guidelines and Pathways cannot specify what should be done for every patient, because there is not strong evidence as to what approach to diagnosis would be most appropriate for some types of patients.30 In addition, the patient may be unwilling or unable to receive the tests recommended by evidence, in which case a different approach will be needed. As a result, physicians must have the ability to depart from the Guideline/Pathway when there are good reasons to do so.31
Accountability for Using Guidelines
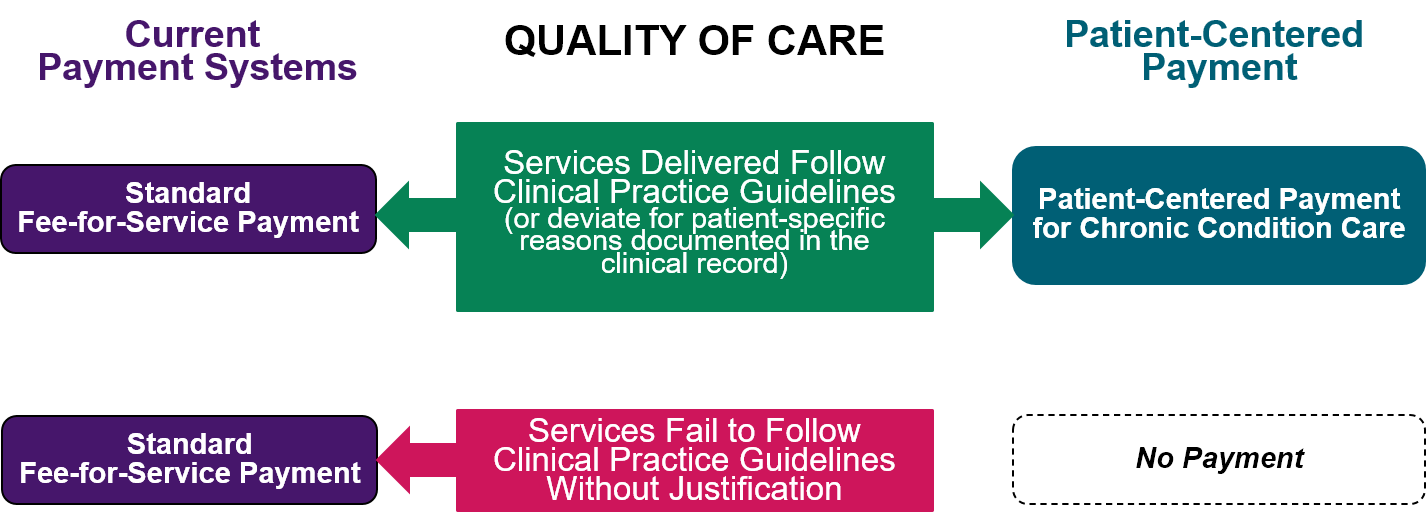
If the specialty practice bills a payer or patient for a Diagnosis Payment, the submission of the bill would mean the physician attested that they had utilized an appropriate Clinical Practice Guideline or Pathway in determining the diagnosis. If the physician deviated from the guidelines, the practice would only submit the bill if the physician attests that the deviation was necessary and the reasons for deviation are documented in the patient’s clinical record.
This is a much stronger standard of quality than exists in current fee-for-service and value-based payment systems. In current payment systems, a physician is paid for performing diagnosis-related activities regardless of whether the activities were supported by evidence or whether all evidence-based steps were followed. Under the patient-centered Diagnosis Payment, there would be no payment at all unless the relevant Clinical Practice Guideline or Pathway was used.
FIGURE 5
Quality Assurance for Diagnosis
Under Current Payment Systems and Patient-Centered Payment
However, the specialty practice should not be expected to submit documentation to a health insurance plan regarding the specific guidelines used or the reasons for deviation in order to receive payment. This is similar to the approach that is used in current fee-for-service payment systems to assure that a physician practice has delivered the service that it is billing for. When the physician practice submits a bill for an office visit, it is attesting that it had the visit with the patient and that the physician spent either a minimum amount of time in conjunction with the visit or that the decision-making in the visit involved a minimum level of complexity. The practice does not have to submit any documentation to the health plan to prove that a visit occurred or that a specific amount of time was spent, but it maintains documentation in the clinical record that can be used, if necessary, to show that the billing was done properly.
While it would obviously be possible for a physician to bill for a Diagnosis Payment without actually following evidence-based guidelines or documenting the reasons for a deviation, it is similarly possible today for a physician to bill for an office visit without actually having delivered it or for delivering a shorter or less complex visit than the bill indicated. If a payer has reason to be concerned that a specialist is not using evidence-based guidelines appropriately, it could request documentation from that practice and recoup any payments that were made inappropriately. This is the same as what is done today in fee-for-service payment systems if there is concern that a physician practice has been billing for services that were not delivered.
Evaluating Diagnostic Accuracy and Improving Diagnosis Guidelines
Using SCAMPs to Develop and Improve Evidence
Use of evidence-based guidelines for diagnosis is an appropriate method of assuring accuracy as long as there is, in fact, evidence that use of the guidelines increases the likelihood of an accurate diagnosis. Although some evidence can be developed through small, controlled studies with selected patients, it should not be assumed that the results will apply to more diverse patient populations without conducting analyses to confirm that. Where there is little or no evidence available, a guideline may not exist or the guideline may not be appropriate for a specific patient. In these cases, physicians will need to deviate from the guidelines or make a diagnosis that is not based on guidelines. However, the accuracy of diagnoses in these cases should ideally be analyzed in order to better guide decisions in the future.
A Standardized Clinical Assessment and Management Plan (SCAMP) is a form of Clinical Practice Guideline/Pathway that is explicitly designed to allow deviations from guidelines in appropriate situations and to use information about the circumstances and reasons for deviations and the outcomes of those choices in order to improve the guidelines.32 SCAMPs have been successfully used to improve guidelines for diagnosis in areas such as evaluating chest pain and diagnosing food allergies.33
Using Registries to Develop and Improve Evidence
In order to use a SCAMP to improve diagnostic accuracy, there has to be a way of obtaining data to help determine whether a diagnosis was accurate or not. In most cases, the data will come from an event that occurs in the future, such as a subsequent evaluation of the patient by the same or a different physician, the results of treatment for the diagnosed condition, the need to treat a complication of an undiagnosed condition, etc.
Analyses of diagnostic accuracy cannot be performed using current healthcare claims data (i.e., the data recorded on the bills physicians submit to health plans for payment) because of the way diagnoses are coded in claims data:
- If a physician determines that a patient does not have a specific disease, there is no way to record that determination when the physician bills for payment, even though it may well be the most desirable outcome of the physician’s evaluation. If the physician rules out one or more diseases as causes of the patient’s symptoms but cannot assign a definitive diagnosis, the billing form will only include codes describing the patient’s symptoms, not any diagnoses that the physician determined do not exist.
- If a patient’s symptoms could be caused by either one disease or a combination of two diseases, and only one disease is coded on a claim form, there is no way to know whether a determination was made that the second disease did not exist or whether the specialist only evaluated the patient with respect to a single disease.
- If the physician determines that the patient could have a particular condition but that a firm diagnosis cannot be made until additional information is available (e.g., until the patient experiences a symptom again or until after the patient receives treatment on a trial basis), there is no way to record that on the claim form. Coding rules require that if a definitive diagnosis cannot be determined, only the symptoms should be recorded.
- If one physician diagnoses a patient with a particular disease, but a second physician determines that the patient does not have the disease, the claims data will indicate that the patient has the disease, because there is no way for the second physician to indicate that the diagnosis code on the initial claim is inaccurate. (The second physician may not even know that the patient was given the diagnosis by a different physician.)
- If one claim is submitted that has a particular diagnosis code, and no subsequent claims have that diagnosis code, it may or may not mean that the patient no longer has the disease or that the patient never had the disease.
A partial solution to this information gap would be to create a billing code modifier that explicitly indicates that the diagnosis codes recorded on the claim form were diagnoses that were excluded, rather than diagnoses that were made. However, there would still be no good way to identify situations in which a definitive determination about a disease was not possible and why.
The most complete information about what was and was not diagnosed and the reasons why is in the patient’s clinical record. If physician practices link their electronic health record systems to a Clinical Data Registry (CDR), relevant portions of the information can be used to analyze diagnostic accuracy and to improve evidence-based guidelines. A CDR is a database that assembles information from multiple physician practices in a way that supports analysis and research on the effectiveness of different approaches to diagnosis and treatment for patients with specific characteristics.
A number of CDRs have been created by medical specialty societies and other groups that are being used for this purpose. For example, the American College of Cardiology’s PINNACLE registry was created in 2008 and has been used for more than a decade to analyze care processes and outcomes for patients with coronary artery disease, hypertension, heart failure, and atrial fibrillation.34 In 2014, the American College of Cardiology, the American College of Physicians, the American Diabetes Association, the American Association of Clinical Endocrinologists and the Joslin Diabetes Center created the Diabetes Collaborative Registry to play a similar role for patients with diabetes and prediabetes.35 The PINNACLE registry and the Diabetes Collaborative Registry are operated in a coordinated way, since many patients have both diabetes and heart conditions and one of the goals of effective treatment of diabetes is to prevent development or exacerbation of heart conditions.
Creating and maintaining registries is an expensive endeavor, both for the specialty societies that manage them and for the physician practices that submit data to them. Many existing registries have been forced to devote most of their time and resources to calculating narrowly-defined quality measures required by pay-for-performance programs in order to make it worthwhile for physicians to participate, rather than expanding and strengthening the evidence for Clinical Practice Guidelines.
Consequently, in order to support a true SCAMP process, Diagnosis Payments need to be large enough to enable specialists to participate in CDRs and to spend the time needed to document not only the reasons for deviations from guidelines but also the outcomes achieved for the patients.
Adequacy of Payment
The third essential characteristic of a patient-centered payment system is that the payment amounts are adequate to cover the cost of delivering services in a high-quality manner. No matter what method is used to pay for diagnosis, if the payment amount is not sufficient to cover the time and cost involved in determining a diagnosis, the patient may fail to receive an accurate diagnosis or may receive harmful or unnecessarily expensive testing.
Challenges in Determining Adequate Payment Amounts
There is very little information available on what it actually costs to determine a diagnosis for a patient. Information is available on how much is currently being paid for visits with physicians, but the payment amounts may or may not be adequate to cover the cost of all of the time spent by physicians and other practice staff in conjunction with the visit. Moreover, the cost of a visit is not the same as the cost of determining a diagnosis. Some patients may need multiple visits in order for a specialist to determine a diagnosis, and they may receive services other than a diagnosis during a visit (e.g., planning of treatment for the diagnosed condition).
It is generally believed that one of the reasons for high rates of diagnostic errors today is that current visit-based payments are inadequate to support effective diagnostic processes.36 Determining what payment amount is adequate requires knowing how much it costs to perform effective diagnostic determinations, but there will not be enough examples of effective diagnosis processes until payments are adequate to support delivering them.
The only way to resolve this “chicken and egg” problem will be to begin using Diagnosis Payments with payment amounts based on best estimates of time and costs (accepting the reality that those amounts may not be exactly right), allow specialists to use the payments to restructure and improve the diagnosis process, gather data on how much time is actually needed to deliver high-quality care, and then refine the amounts over time as those data become available. This process will likely take several years to complete. This is similar to what is done in the current fee-for-service payment system. Each year, CMS adjusts the Medicare payment amounts for various physician services based on new information and evidence about the cost of delivering the services to patients.
Estimated Amounts for Diagnosis Payments
An estimate of the amount needed to support adequate time for diagnosis can be made by (1) estimating the cost of operating a hypothetical specialty practice that exclusively performs diagnoses on patients with symptoms relevant to that specialty, (2) estimating the amount of time involved in carrying out the processes associated with the three different levels of diagnostic complexity associated with the Diagnosis Payments, and then (3) calculating the cost for the specialty practice to spend that amount of time.
The Cost of Operating a Specialty Practice
Figure 6 shows a hypothetical specialist practice and what it might cost to operate such a practice.
FIGURE 6
Cost of Operating
a Small Specialist
Physician Practice
| Practice Expenses | |
| Physician | $250,000 |
| Medical Assistant | $38,000 |
| Receptionist | $36,000 |
| Billing | $18,000 |
| Benefits | $48,400 |
| Total Personnel | |
| Rent/Utilities | $40,000 |
| EHR and IT | $10,000 |
| Liability Insurance | $6,000 |
| Supplies/Other | $10,000 |
| Total Non-Staff Overhead | $66,000 |
| Total Expenses | $456,400 |
| Physician Time | |
| Weeks Worked Per Year | 48 |
| Hours Worked Per Day | 9.5 |
| Administrative Time | 0.5 |
| Patient Hours | 9.0 |
| Cost per patient hour | $211 |
- The practice has a single physician. In many parts of the country, there are too few patients to support more than one specialist, so it is desirable to design a payment system that will support solo physician practices as well as larger practices. Moreover, it is reasonable to assume that the costs for practices with multiple physicians will be roughly proportional to the number of physicians.37 Although there are some economies of scale for practices with two or more physicians, the savings are limited, and there is also evidence of diseconomies of scale with large practices as well as the potential for higher prices and greater challenges in delivering quality care.38
- The physician employs three people: a full-time medical assistant, a full-time receptionist/office manager, and someone to do billing on a part-time basis.
- The physician is paid $250,000 per year. Many specialists earn more than this, but the amounts vary significantly by specialty and region.39 Since relatively few specialists earn less, this represents a lower bound on this component of the cost of the practice.
- Other staff are assumed to be paid salaries comparable to national averages for those positions.40 In addition to salaries, the physician and staff are assumed to receive health coverage and other basic benefits.41
- The practice rents office space and it pays for computer equipment, an Electronic Health Record (EHR), malpractice and liability insurance, and office supplies and equipment. The amounts a physician practice would need to spend on these things can vary significantly depending on the community where it is located and other factors, so the actual costs for an individual practice may be higher or lower than the amounts assumed here. However, since these items represent a small portion of the total practice expenses, differences in the costs will have a limited impact on the overall cost estimate.
Using these assumptions, the total annual cost of operating the hypothetical practice will be about $460,000, slightly less than twice the salary paid to the physician. If the specialist earns or is paid a higher salary, the total cost would be higher by a corresponding amount.
As shown in Figure 6, if one assumes the physician works 48 weeks per year and spends 9 hours per day on activities related to patient diagnoses, the cost of time spent on diagnostic activities is $211 per hour.
Obviously, most specialists will not spend their time exclusively performing diagnoses. However, if only a portion of the physician’s total time is spent determining diagnoses, then a corresponding portion of the practice cost should be assigned to diagnostic services, and the hourly cost would remain the same.
Estimated Cost of Diagnosis
In order to use the cost per hour information from Figure 6 to determine amounts for the payments in Figure 4, estimates must be made for the amount of time the physician will spend performing the services associated with each payment.
Figure 7 assumes that at least 30 minutes with the patient should be allocated for any set of symptoms that meet the minimum threshold for a diagnostic visit with the specialist and that an additional 15 minutes is required for each higher level of complexity. This time might be spent in a single visit or multiple visits; for example, if a moderate complexity diagnosis requires an initial 30-minute visit followed by additional testing, and then the final determination is made in a second 15-minute visit, the total time spent would be 45 minutes.
FIGURE 7
Estimated Time and Payment Amounts for Specialist Diagnosis Services
| Code | Diagnosis Services | Time with Patient (Minutes) | Documentation & Coordination with Primary Care (Minutes) | Total Time (Minutes) | Estimated Cost | Margin | Payment Amount |
|---|---|---|---|---|---|---|---|
| XX040 | Diagnosis Assistance | 0 | 10 | 10 | $35 | 3% | $37 |
| XX041 | Low Complexity Diagnosis | 30 | 10 | 40 | $141 | 3% | $146 |
| XX042 | Moderate Complexity Diagnosis | 45 | 15 | 60 | $211 | 3% | $218 |
| XX043 | High Complexity Diagnosis | 60 | 20 | 80 | $282 | 3% | $291 |
It is also assumed that an additional 10-20 minutes will be needed beyond the time with the patient to document the findings and communicate them to the patient’s primary care physician, with longer amounts of time required for more complex determinations.
If the specialist is providing assistance to a primary care physician in making a diagnosis or determining whether to refer the patient to the specialist, it is assumed there would be no direct time spent with the patient, but instead that up to 10 minutes would be spent in the interaction between the specialist and the primary care physician.
Based on these assumptions, Figure 7 shows estimated payment amounts determined by multiplying these time estimates by the hourly cost shown in Figure 6 and adding a small (3%) margin. As noted earlier, if the specialist earns a higher annual salary, then the hourly cost of the practice would be higher and the payment amounts would need to be correspondingly higher.
If data become available showing that more time is needed for one or more of these categories of diagnosis services, the payment amounts should be revised accordingly. However, physicians should not be required to spend the exact amount of time shown in order to be paid for the corresponding service to an individual patient. If a specialist can perform the tasks needed for a particular service in a shorter amount of time, they should be still be paid the standard amount for that service. This will offset the higher-than-average amounts of time spent with other patients.
Patient Access and Choice
A patient should be able to receive diagnostic services from the physician(s) best able to diagnose their symptoms accurately and safely. Many patients will be able to obtain an accurate diagnosis from their primary care physician, while others will need to see a specialist even after seeing a primary care physician. No one specialist will be best at diagnosing all types of patients, even if the patients have similar symptoms, and some patients may need to see multiple specialists when they have symptoms that can result from several different kinds of diseases or conditions.
In many health insurance plans, patients can only receive full coverage for services if the services are delivered by physicians who are part of a payer-defined network. The network is typically defined based primarily on the fee the physician will accept, rather than the specific types of expertise they have or the quality of care they will provide. In addition, many insurance plans have prior authorization systems that may deny coverage for specific services even if they are delivered by physicians who are “in-network.” Neither of these approaches is consistent with patient-centered care and they can prevent patients from receiving the services they need from the physicians best able to deliver them.
Also, most health insurance plans require patients to pay a co-payment or co-insurance in order to see a specialist, and a patient may need to pay the full cost of the visit if they have not yet paid for enough services during the year to meet the deductible required under their insurance plan. Although requiring patients to pay these various forms of cost-sharing may discourage them from making unnecessary visits to specialists, it can also discourage patients from seeing a specialist when that is necessary for determining an accurate diagnosis. Since inaccurate diagnoses can lead to higher-than-necessary spending on treatments for the wrong disease and for complications resulting from an undiagnosed disease, it can be “penny-wise and pound-foolish” to require cost-sharing for high-quality diagnostic services.
A patient-centered approach to cost-sharing should:
- Encourage primary care-based diagnosis whenever possible. Ideally, a patient who is enrolled with a primary care practice would seek help from that practice first when they have new (non-emergency) acute symptoms. Many symptoms can be correctly diagnosed by a primary care physician, and primary care physicians will be better able to diagnose symptoms accurately if (1) the primary care practice is receiving Patient-Centered Primary Care Payment that allows the physician to spend adequate time on new acute problems, and (2) specialists can receive a Diagnosis Assistance Payment for helping the primary care practice make accurate diagnoses and referrals.
- Enable diagnostic consultations with specialists when needed. If the primary care practice determines that an evaluation by a specialist is needed for an accurate diagnosis, there should be not be a financial barrier to the patient obtaining such an evaluation. In some cases, even if the primary care physician does not think a specialist evaluation is necessary, the patient may be concerned that the diagnosis they received is inaccurate; if so, it would be desirable for the patient to receive a second opinion from an appropriate specialist. If the patient’s symptoms could be due to two or more very different health problems, they may need to see two or more specialists until the cause is identified.
- Encourage accurate diagnosis for complex symptoms. If a patient has a more complex or difficult-to-diagnose set of symptoms, the payment to the physician will need to be higher because the physician will need to spend more time on the patient’s case. However, the patient should not have to pay more in cost-sharing, since the higher cost and/or uncertainty about the cost-sharing amount could deter them from obtaining an accurate diagnosis.
- Discourage unnecessary diagnostic evaluations. If a physician has determined that a patient has (or does not have) a particular condition, and that diagnosis has been confirmed by a second physician, there will likely be little value in additional diagnostic evaluations by other physicians, so the patient should pay more if they want such evaluations.
The following approach to cost-sharing would support these goals:
- The cost-sharing should be lower for an initial evaluation of symptoms by a primary care physician rather than a specialist.
- There should be no cost-sharing for a diagnostic assistance payment to a specialist who assists the primary care physician in making a diagnosis or determining whether a specialist referral should be made.
- There should be no cost-sharing for a visit to a specialist if the patient has visited a primary care physician or a specialist who was unable to make a diagnosis.
- There should be low cost-sharing for a visit with a specialist if a primary care physician has made a diagnosis but the patient wants a second opinion.
- The cost-sharing amounts should be higher for subsequent specialist evaluations of the same symptoms after a diagnosis has already been made by one specialist.
- The dollar amount of cost-sharing for the patient should be the same regardless of the level of Diagnosis Payment paid to the specialist.
For example, if the cost-sharing for an Acute Care Visit under Patient-Centered Primary Care Payment is $25, then the cost-sharing for a Diagnosis Payment to a Specialist could be $50, unless the patient has had an Acute Care Visit with a primary care physician for the same symptoms within the previous 30-60 days that did not result in a diagnosis, or the patient cannot afford the cost-sharing amount, in which case the cost-sharing should be $0. Figure 8 shows an example of a cost-sharing structure consistent with this approach.
FIGURE 8
Patient Cost-Sharing for Diagnosis Payments
| Service and Circumstances | Previous Visit with PCP? | Previous Visit with a Specialist? | Example of Patient Cost-Sharing |
|---|---|---|---|
| Acute Care Visit with Primary Care Physician (PCP) | N/A | N/A | $25 co-pay |
| Diagnostic Assistance to PCP by Specialist | N/A | N/A | $ 0 co-pay |
| Diagnosis Payment to Specialist | Visit that did not result in a diagnosis | No previous visit for same symptoms | $ 0 co-pay |
| Visit that did not result in a diagnosis | Previous visit that did not result in a diagnosis | $ 0 co-pay | |
| No PCP visit for same symptoms | No previous visit for same symptoms | $50 co-pay | |
| PCP visit that resulted in a diagnosis | No previous visit for same symptoms | $25 co-pay | |
| N/A | Previous visit that resulted in a diagnosis | 100% of payment |
Payment for Care Planning
Although some patients who see a specialist for diagnosis of symptoms will want or need to receive a care plan from that specialist, that will not be true in all cases:
- If the specialist determines the patient does not have a chronic disease, there may be no need for treatment or care at all.
- The patient’s primary care physician may be able to develop an appropriate care plan for the patient once a diagnosis is determined. Indeed, if the primary care physician is already providing care for other health issues, they may be in a better position to develop a care plan that appropriately complements the patient’s other treatments.
Conversely, the primary care physician may have been able to accurately diagnose the patient’s condition, but a specialist may need to develop a care plan because of the complexity of the patient’s condition or the complexity of the treatment options available.
In some cases, the specialist who prepares the care plan may be different from the specialist who diagnoses the patient’s condition. For example, this could occur if the patient has been diagnosed by a subspecialist in a distant community but will be treated by a specialist in their home community or if a subspecialist in a different community is asked to develop an appropriate treatment plan for a complex patient.
In order to ensure that the clinician who develops a care plan for a patient is paid adequately for doing so, there need to be Care Planning Payments that are separate from the Diagnosis Payments used to support the diagnostic process.
Method of Payment
Problems with Current Payments
Currently, there are no billing codes or fees specifically designed to pay a specialty care practice to identify appropriate treatment options for a patient’s disease and work with the patient to develop a plan for managing that disease. As with diagnosis, the work involved in care planning is currently paid for using the generic “Evaluation and Management Services (E/M)” fees that are triggered by a visit between the patient and the physician. However, because the payment is for an “office visit,” the payment may not be adequate to support an appropriate care planning process and there is no assurance that payment will result in a clear plan of care that will be feasible for the patient to follow.
A Patient-Centered Approach to Payment for Care Planning
In a patient-centered approach to payment, a physician practice should receive a Care Planning Payment specifically designed to support development of an appropriate care plan for the patient. The physician practice would only bill for a Care Planning Payment when a care plan tailored to the patient’s needs has been completed and documented for an individual patient. If the care planning process requires multiple visits or contacts with the patient, there should be one Care Planning Payment that reflects the total expected time for those visits, instead of separate fees paid for each visit. If the care planning process can be carried out effectively through telehealth, the Care Planning Payment should be paid even if there was no in-person visit with the patient.
Care Planning Payments must be adequate to support the time required to identify the most current evidence available about the effectiveness of alternative treatment approaches and to engage in a shared decision-making process with the patient in determining the best approach to treatment.
Stratifying Payments Based on the Complexity of Care Planning
More time will be needed to carry out an effective care planning process for some patients than others:
- Multiple options for treatment and management. If there are multiple medications or treatment options available, there may be tradeoffs between effectiveness in controlling symptoms, problematic side effects, and/or cost that patients will need to understand in order to make an informed choice.
- Treatments requiring customization based on patient characteristics. Some types of treatment will be more effective or more problematic for patients who have particular genetic characteristics, comorbidities, etc. that require additional testing to evaluate.
- Barriers to use of treatments and/or self-management. Some patients may not be able to afford certain treatments or may require extra support to carry out self-management tasks. Efforts will be needed to obtain additional assistance for them before a care plan can be finalized.
- Challenges in understanding treatment options. Some patients may have cognitive limitations or language/literacy barriers that make it difficult for them to understand treatment options. They will require additional time from the physician or other practice staff.
The evaluation and management services (E/M) payments currently used to pay for office visits are stratified based on two criteria: (1) the complexity of the “medical decision-making,” and (2) the amount of time the physician spends on the patient’s case, including time spent outside of the face-to-face visit with the patient. As shown in Figure 9, the criteria used for determining complexity of medical decision-making are applicable to care planning as well as diagnosis, except that the first criterion would be determined by the number of management options being evaluated (rather the number of diagnoses being considered).42 Since it is unlikely that patients in the straightforward decision-making category would require care planning from a specialist rather than their primary care practice, the three higher categories of complexity (low, moderate, and high) could be used in stratifying the Care Planning Payments in a patient-centered payment system.
FIGURE 9
Classification of Medical Decision-Making Complexity
for Current Evaluation and Management Services Payments
| Level of Medical Decision-Making | Two of the Following Three Criteria: | ||
|---|---|---|---|
| Number of Management Options | Amount and/or Complexity of Data Reviewed | Comorbidities and Complications | |
| Straightforward | Minimal | Minimal or None | Minimal |
| Low Complexity | Limited | Limited | Low |
| Moderate Complexity | Multiple | Moderate | Moderate |
| High Complexity | Extensive | Extensive | High |
In contrast, the time criterion that is used to stratify E/M payments is problematic for the purposes of care planning, since it is defined only in terms of time spent by the physician. Patients who require more time in order to understand the differences in treatment options may benefit most from spending that time with a nurse or another member of the practice staff, not with the physician. Moreover, the cost of the nurse’s time would be significantly lower than the cost of having the physician spend the time. To address this, a separate payment could be made for patients who need additional time, with the payment amount based on the cost of a nurse’s time rather than a physician’s time.
Under this approach, there would be three levels of Care Planning Payment based on the complexity of medical decision-making, and a fourth payment that would be paid in addition to the others for patients who require additional time and assistance from the staff of the physician practice rather than the physician:
- Low Complexity Care Planning Payment
- Moderate Complexity Care Planning Payment
- High Complexity Care Planning Payment
- Payment for Additional Care Planning Time by Clinical Staff (15 minutes)
Payment for Assistance to Primary Care Physicians
If a primary care practice will be providing ongoing care for the condition or if it is already treating the patient for other conditions, it may be best for that practice to take the lead in developing a care plan for the patient’s chronic condition even if the condition has been diagnosed by a specialist. However, the primary care physician may need assistance from a specialist to identify all of the current treatment options available and to determine which would be most appropriate for the patient. Providing this assistance to the primary care physician requires some of the specialist’s time, but not as much time as the specialist would need to spend to develop a care plan themself.
To support this, a Care Planning Assistance Payment should be created to enable the specialist to provide assistance to a primary care physician in developing a care plan for patient.43
Billing and Payment for Care Planning Services
This approach to paying for care planning can be easily operationalized for patients who have insurance by creating five new billing codes. As shown in Figure 10, each of the five categories of services would be assigned either a CPT® (Current Procedural Terminology) code by the American Medical Association’s CPT Editorial Panel or a HCPCS (Healthcare Common Procedure Coding System) Level II code by the Centers for Medicare and Medicaid Services (CMS) HCPCS Workgroup.
FIGURE 10
Payments for Specialty Care Planning Services
| CPT/HCPCS Code | Payment Category | Service |
|---|---|---|
| XX050 | Care Planning Assistance Payment | Assistance to a primary care practice in developing a care plan |
| XX051 | Low Complexity Care Planning Payment | Development of a care plan requiring low-complexity decision-making |
| XX052 | Moderate Complexity Care Planning Payment | Development of a care plan requiring moderate-complexity decision-making |
| XX053 | High Complexity Care Planning Payment | Development of a care plan requiring high-complexity decision-making |
| XX054 | Payment for Additional Care Planning Time | Significantly higher time spent by practice staff to assist a patient in making decisions about their care plan |
The physician who is developing the care plan would choose the appropriate CPT/HCPCS code(s) based on (1) the complexity of the planning required in light of the number and types of treatment options available and the patient’s characteristics, and (2) whether the patient needed significantly more time and assistance by practice staff in order to understand and choose among the options available.
If a physician practice bills for one of these codes for a patient, it would not bill for an E/M payment for any visits that patient made as part of the care planning process.
Payment for Additional Diagnostic Testing
The Care Planning Payment would support the time spent by the physician and other practice staff in working with the patient to develop a plan of treatment for the patient’s condition. If the physician needs the results of additional laboratory tests or imaging studies in order to determine the appropriate type of treatment, separate payments will need to be made for those tests.
Accountability for Quality and Utilization
Problems with Current Approaches
Care planning has become increasingly time-consuming for physician practices and frustrating for both physicians and patients because of rules and requirements imposed by health insurance plans, such as prior authorization (requiring approval from the health plan before a particular treatment can be used), step therapy (requiring a less expensive treatment to be used before a more expensive treatment can be used), and formularies and narrow networks (which limit the types of drugs or specific providers that can be used to deliver treatments). In some cases, these programs may prevent patients from receiving inappropriate or unnecessary treatments, but in many cases, they either delay or prevent patients from receiving the most appropriate treatments, and this can harm the patient. Moreover, these approaches have significantly increased administrative costs for both physician practices and health plans, with no evidence that they have resulted in equivalent or greater reductions in spending on treatments or in improvements in patient outcomes.
Use of Clinical Practice Guidelines
The best way to ensure that patients are receiving the most appropriate treatment for their condition is for physicians to utilize evidence-based Clinical Practice Guidelines (CPGs) in identifying the treatment options that would be appropriate for a particular patient. A Clinical Practice Guideline assembles all of the available evidence regarding how to treat a particular condition, with consideration for the tradeoffs between effectiveness and safety.44 Evidence-based Clinical Practice Guidelines exist for treatment of most common chronic diseases and symptoms and also for many less-common conditions. The same guidelines described in Section 3.C.2.b for diagnosis of asthma, COPD, diabetes, heart failure, ischemic heart disease, and other conditions also include guidelines for how to treat these conditions, and strong efforts are made to ensure that guideline recommendations are based on what is best for patients.
Since Clinical Practice Guidelines define which treatments are appropriate in various situations, they can reduce use of unnecessary and inappropriate treatment in a more patient-centered way than the burdensome and problematic prior authorization processes typically used by health insurance plans. In order to reduce variation when there are multiple treatment choices and the available evidence does not indicate which option is better, a recommended option can be added to the guidelines. As discussed earlier in conjunction with diagnosis, the term “Clinical Pathway” is often used to describe a set of guidelines that recommend the use of a specific approach when the evidence is unclear or where multiple options have equivalent benefit but different costs.45
To be successful, CPGs and Pathways must be developed and refined by clinicians, not by health plans. Clinicians will be more likely to utilize and adhere to clinician-developed guidelines than rules or pathways developed by payers or other entities where cost considerations may have taken precedence over patient outcomes in defining recommendations.46 In addition, a CPG developed by clinicians can be used for all patients, regardless of payer.
Guidelines and Pathways cannot specify what treatment is appropriate for every patient, however, because there is not strong evidence as to what approach to treatment would achieve the best result for some types of patients.47 In particular, when patients have multiple chronic conditions, guidelines designed for care of individual diseases may not be appropriate. In some cases, the patient may be unwilling or unable to accept the services recommended by evidence, and a different set of services will be needed. As a result, physicians must have the ability to deviate from a Guideline or Pathway in developing a care plan when there are good reasons to do so.48
However, as previously discussed in Section 3.C.2.d with respect to diagnosis, a process is needed to assess the situations in which these deviations occur and the resulting outcomes in order to determine whether and how the Guideline/Pathway should be revised. If physician practices link their electronic health record systems to a Clinical Data Registry (CDR), relevant portions of the information can be used to carry out this process. The Care Planning Payments need to be large enough to enable specialists to participate in CDRs and to spend the time needed to document outcomes for patients.
Shared Decision-Making With Patients
Even if guidelines indicate that a particular treatment would be appropriate for a patient, the decision to incorporate it into a patient’s care plan should generally only be made after engaging in a shared decision-making process with the patient. In a shared decision-making process, the patient receives information that objectively describes the treatment options available in a way they can understand and that explains the advantages and disadvantages of each option based on criteria relevant to the patient, including cost to the patient, risks of side effects or injury, effectiveness in enabling the patient to perform activities important to them, etc.49 If the patient cannot or should not make a decision based on that information alone, the patient should be asked to express their personal goals and preferences so the physician can make recommendations for treatment based on those goals and preferences. The physician and patient should then reach agreement on what the care plan should be.
Written Care Plans
In most cases, optimal care for a chronic disease will involve multiple activities, including lifestyle changes by the patient as well as taking medications or receiving other types of treatment. It may be difficult for patients to accurately remember all of these activities without a written list and description of each activity, particularly if they need to occur at specific times or be carried out in specific ways. Consequently, the patient should receive a written care plan. (CMS requires a written care plan in order for physician practices to bill for Chronic Condition Management (CCM) payments.)
In addition, the severity of a chronic disease exacerbation and associated complications can often be reduced if specific actions are taken by the patient when symptoms of the exacerbation first appear, such as contacting their physician’s office immediately in order to receive a different medication or a different dosage of an existing medication. Since these situations will (hopefully) occur infrequently, it will be difficult for many patients to remember exactly what the appropriate response is when the situation does occur unless the patient has a written reference they can consult. These are often referred to as “action plans” and can be part of the written care plan. For example, the Guidelines for the Diagnosis and Management of Asthma developed by the National Asthma Education and Prevention Program recommend that every patient receive a “written asthma action plan that includes two aspects: (1) daily management and (2) how to recognize and handle worsening asthma.”50
Accountability for Using Guidelines and Shared Decision-Making
In order for a specialty practice to bill a payer or patient for one of the Care Planning Payments listed in Figure 10, the physician should attest that they:
- utilized an appropriate Clinical Practice Guideline or Pathway to identify appropriate treatment options;
- engaged in a shared decision-making process with the patient to select a particular approach to treatment and management of the condition (including a decision not to treat the condition at all); and
- prepared a written care plan and provided a copy of it to the patient.
If the care plan deviated from Clinical Practice Guidelines, the practice should only submit the bill if the physician attests that the deviation was necessary or appropriate for patient-specific reasons and that the reasons for the deviation are documented in the patient’s clinical record. However, the practice should not be expected to submit documentation to the health insurance plan regarding the specific guidelines used or the reasons for deviation in order to receive payment.
This is similar to the approach that is used in current fee-for-service payment systems to assure that a physician practice has delivered the service that it is billing for. When the physician practice submits a bill for an office visit, it is attesting that it had the visit with the patient and that the physician spent either a minimum amount of time in conjunction with the visit or that the decision-making in the visit involved a minimum level of complexity. The practice does not have to submit any documentation to the health plan to prove that a visit occurred or that a specific amount of time was spent, but it maintains documentation in the clinical record that can be used, if necessary, to show that the billing was done properly.
While it would obviously be possible for a physician to bill for a Care Planning Payment without actually following evidence-based guidelines or engaging in a shared decision-making process with the patient, it is similarly possible today for a practice to bill for an office visit without actually having delivered it or for delivering a shorter or less complex visit than the bill indicated. If a payer has reason to be concerned that a particular specialist is not developing care plans appropriately, it could request documentation from that practice and recoup any payments that were made inappropriately. This is the same as what is done today in fee-for-service payment systems if there is concern that a practice has been billing for services that were not delivered. The best method of ensuring that specialty practices engage in shared decision-making with patients and provide them written with care plans is to make sure that patients understand that they should expect to receive a written care plan and to have been involved in the process of developing it.
Adequacy of Payment
As with diagnosis, having a good method of paying for care planning is necessary but not sufficient. The amount of the Care Planning Payment has to be sufficient to cover the time and cost involved in consulting Clinical Practice Guidelines, engaging in a shared decision-making process, and preparing a written care plan.
Challenges in Determining Adequate Payment Amounts
As with diagnosis, there is very little information available on what it actually costs to develop a care plan for a newly-diagnosed chronic condition. One of the barriers to engaging in shared decision-making processes with patients and preparing written care plans is that payments for office visits are not adequate to support the time needed to engage in these processes, particularly when much of the work can and should be done by nurses who cannot directly bill for services and whose time is not currently counted in determining which fee can be billed. It will be impossible to know exactly how much time is required to carry out these tasks until payments are adequate to support performing them.
The only way to resolve this “chicken and egg” problem will be to begin using Care Planning Payments with payment amounts based on best estimates of time and costs (accepting the reality that those amounts may not be exactly right), allow specialists to use the payments to restructure and improve the care planning process, gather data on how much time is actually needed to develop care plans properly, and then refine the payment amounts over time as those data become available. This process will likely take several years to complete. This is similar to what is done in the current fee-for-service payment system. Each year, CMS adjusts the Medicare payment amounts for various physician services based on new information and evidence about the cost of delivering the services to patients.
Estimated Amounts for Care Planning Payments
A method of estimating the cost of time spent on a service by a specialist physician was developed in Section 3.C.3 in conjunction with Diagnosis Payments. In order to estimate the cost of care planning, an estimate is also needed of the cost of time spent by a nurse, as well as estimates of the amounts of time the physician and nurse would spend carrying out the processes associated with each of the Care Planning Payments.
The Additional Cost of Employing a Nurse
FIGURE 11
Cost of Employing
Nursing Staff
in a Small
Specialist Practice
| Additional Practice Expenses | |
| Registered Nurse | $80,000 |
| Benefits | $16,000 |
| Total Personnel | $96,000 |
| Rent/Utilities | $5,000 |
| EHR and IT | $4,000 |
| Liability Insurance | $3,000 |
| Supplies/Other | $2,000 |
| Total Non-Staff Overhead | $14,000 |
| Total Expenses | $110,000 |
| Nurse Time | |
| Weeks Worked Per Year | 50 |
| Hours Worked Per Day | 8.0 |
| Administrative Time | 0.5 |
| Patient Hours | 7.5 |
| Cost per patient hour | $59 |
Figure 11 shows what it might cost to employ a nurse at a hypothetical physician practice in addition to the other staff and expenses shown in Figure 6. It is assumed that the nurse is paid a salary comparable to national averages51 and receives health coverage and other basic benefits.52 The practice is assumed to require additional office space for the nurse, additional computer equipment and software for carrying out the nurse’s functions, additional malpractice and liability insurance, and additional office supplies and equipment. The amounts a physician practice would need to spend on these things can vary significantly depending on the community where it is located and other factors, so the actual costs for an individual practice may be higher or lower than the amounts assumed here. If one assumes the nurse works 50 weeks per year and spends 7.5 hours per day on activities related to patient care planning, the cost of time spent on these activities would be $59 per hour.
Obviously, a nurse at a specialty practice will not spend all of their time performing activities related to care planning. However, if only a portion of the nurse’s total time is spent in this way, then a corresponding portion of the cost of the nurse should be assigned to care planning services, and the hourly cost would remain the same.
Estimated Cost of Care Planning
In order to use the cost per hour information from Figures 6 and 11 to determine amounts for the payments in Figure 10, estimates must be made for the amount of time the physician and nurse will spend performing the services associated with each payment.
Figure 12 assumes that at least 10 minutes of the physician’s time would be needed for any care plan and that an additional 10 minutes would be required for each higher level of complexity in choosing treatment options. It is also assumed that an additional 5-15 minutes will be needed for the physician to document the treatment approach chosen in the clinical record and to communicate it to the patient’s primary care physician, with longer amounts of time required for more complex plans.
FIGURE 12
Estimated Time and Payment Amounts for Care Planning Services
| Code | Care Planning Services | Physician Time with Patient (Minutes) | Nurse Time with Patient (Minutes) | Physician Documentation & Coordination with Primary Care (Minutes) | Written Care Plan (Nurse Minutes) | Total Time (Minutes) | Estimated Cost | Margin | Payment Amount |
|---|---|---|---|---|---|---|---|---|---|
| XX050 | Care Planning Assistance | 0 | 0 | 10 | 0 | 10 | $35 | 3% | $37 |
| XX051 | Low Complexity Care Planning | 10 | 10 | 5 | 10 | 35 | $72 | 3% | $75 |
| XX052 | Moderate Complexity Care Planning | 20 | 20 | 10 | 15 | 65 | $140 | 3% | $145 |
| XX053 | High Complexity Care Planning | 30 | 30 | 15 | 20 | 95 | $207 | 3% | $214 |
| XX054 | Additional Care Planning Time | 0 | 30 | 0 | 0 | 30 | $29 | 3% | $31 |
It is assumed that the amount of time the nurse spends assisting the patient to understand the tradeoffs among the treatment options would be equivalent to the time the physician is spending on identifying the treatment options for the patient and explaining them, and that the nurse will also spend an additional 10-20 minutes preparing a written care plan. For patients who require significantly more time, it is assumed that the nurse would spend an additional 30 minutes.
If the specialist is providing assistance to a primary care physician in developing a care plan, it is assumed there would be no direct time spent with the patient by either the specialist or nurse, but instead that up to 10 minutes would be spent in the interaction between the specialist and the primary care physician.
Based on these assumptions, Figure 12 shows estimated payment amounts determined by multiplying these time estimates by the hourly costs shown in Figure 6 and Figure 11 and adding a small (3%) margin. As noted earlier, if the specialist earns a higher annual salary, then the hourly cost of the practice would be higher and the payment amounts would need to be correspondingly higher.
If data become available showing that more (or less) time is needed for these different categories of care planning services, the payment amounts should be revised accordingly. However, physicians and nurses should not be required to spend the amount of time shown in order to be paid for the corresponding service to an individual patient. If the staff in a physician practice can perform the tasks needed for a particular service in a shorter amount of time, they should still be paid the standard amount for that service.
Patient Access and Choice
A patient who has been newly diagnosed with a chronic condition should have a physician practice with the appropriate expertise develop an evidence-based care plan for that condition. Requiring a patient to pay cost-sharing could discourage them from obtaining such a care plan and result in them receiving inadequate or inappropriate treatment for their condition. Consequently, once the patient has been diagnosed with a chronic condition, there should be no cost-sharing required for the development of a care plan by either their primary care practice or a specialist practice.
Payment for Condition Management
Method of Payment
Monthly Payments for Proactive Care
Development of a care plan will trigger the beginning of what will often be a lifetime of activities needed to manage the chronic disease, including both treatments and lifestyle changes designed to reduce the severity of symptoms caused by the chronic condition, to prevent exacerbations of the condition and associated complications, and ideally to slow the progression of the disease.
- Most patients will need education and assistance from a physician practice in order to successfully implement a care plan and adhere to it over time.
- Many patients will need prescription medications to manage their condition, and they may need advice and assistance from a physician practice about how to take the medications appropriately and how to identify and respond appropriately to any problematic side effects. Some medications can have serious side effects that require careful monitoring and rapid response when problems occur. In some cases, the medications will have to be administered in the physician’s office, while in other cases, the patient will obtain their medications from a community pharmacy. Different approaches to education, symptom monitoring, and response to side effects will be needed depending on all of this.
- Even with the most effective treatment plan, some patients will experience exacerbations of their condition during the course of the year, and it will be important for their physician practice to identify those exacerbations as quickly as possible and take appropriate action in order to avoid more serious problems from occurring. In some cases, this will require a face-to-face visit with the patient, and in other cases, a phone call or telehealth visit will suffice.
- The patient’s care plan will need to be adjusted from time to time as the patient’s needs change and as new evidence about the effectiveness of alternative treatments becomes available.
This combination of education, assistance, monitoring, response to problems, and adjustments to care plans must be continuous and proactive. The services needed cannot be delivered effectively solely through office visits with the physician; patients need to be contacted between visits in order to prevent problems from occurring and to respond quickly when problems occur. In addition, although development and adjustments to a treatment plan for a chronic condition must generally be done by a physician or other clinician, services such as education, assistance, and monitoring can usually be performed primarily by nurses or other types of staff in the physician practice.
As a result, effective management of chronic conditions cannot be supported by typical fee-for-service payments for office visits. Moreover, it is problematic to pay the practice for an office visit when an exacerbation occurs (as is the case in current payment systems), because the practice is then penalized financially when it is able to prevent exacerbations from occurring.
The most appropriate way to pay for chronic condition management is through a monthly Condition Management Payment for each patient that gives the physician practice flexibility to assist each patient in the way that will be most effective and efficient for that patient. A monthly payment also encourages preventing exacerbations and avoiding treatment complications, since the fewer problems the patient has, the less time the practice will need to spend addressing such problems. The monthly payment would only be for chronic condition management, not for any specific drugs, procedures, or tests the patient needs as part of their care plan; these other services should be paid for through service-specific fees.
Patients Eligible for Chronic Condition Management Payments
A patient with any chronic disease that requires a significant amount of proactive care should be eligible for a Condition Management Payment. This would include diseases such as asthma, COPD, diabetes, epilepsy, and rheumatoid arthritis, as well as chronic conditions that often do not receive appropriate attention, such as chronic migraines, depression, and osteoarthritis. In addition, conditions such as obesity, smoking, and substance abuse should be included since they will require proactive management over an extended period of time.
Trying to precisely define which conditions qualify for the payment will only add administrative burden for physician practices and payers, and will be unlikely to lead to better quality care. It would be better to be inclusive initially, and then later exclude specific types of conditions if they are being used as the basis for billing for Condition Management Payments when no significant regular or proactive services are provided or needed. If there is evidence that a physician practice is abusing this flexibility, that practice could be excluded from the Patient-Centered Payment system rather than over-complicating the system for practices that are using it appropriately.
Physician Practices Eligible for Condition Management Payments
Patients should have the ability to choose which physician practice will help them in managing their chronic condition. Some patients will want or need their primary care practice to do this. Other patients will want or need to have a specialist practice do so, even if the patient continues to receive wellness care and occasional acute care from the primary care practice. There are multiple reasons for this:
- In some cases, the patient’s primary care practice may not have the expertise or resources to appropriately manage the patient’s chronic condition(s), particularly if the patient has a severe or unusual form of the condition(s) or if standard treatments are not effective or have problematic side effects, and so ongoing chronic condition management by a specialist practice will be necessary.
- In other cases, a specialist practice may need to provide services initially until an effective treatment and management plan is identified, and then a primary care practice can deliver the services under the plan on an ongoing basis.
- In still other cases, a specialist practice that diagnosed the patient’s condition or developed a care plan for it may not be able to provide ongoing management of the patient’s condition even if it were desirable for it do so, e.g., if the specialist practice is located in a different city or if it does not have the capacity to take on management of an additional patient, and so the patient’s primary care practice will need to provide the care for the condition on an ongoing basis.
- Some patients who are receiving chronic condition management services from a primary care practice may need to temporarily receive those services from a specialty practice rather than the primary care practice, such as when the patient experiences an acute condition that complicates management of the chronic condition (e.g., the patient becomes pregnant and the medications she had been taking for the chronic condition would be problematic to continue using during her pregnancy).
- A patient might need to switch temporarily from one physician practice to another for a period of time, such as when the patient is temporarily living in a different community. In these cases, the patient can stop receiving chronic condition management services from their primary care practice or their current specialty care practice and then begin receiving them again when the reason for the change has ended. Since the payments are monthly, a physician practice can receive the monthly payments for a particular patient only during the months when the practice is actually providing the services to that patient.
The best way to determine which physician practice has responsibility for providing condition management services to a patient is to have the patient explicitly enroll with that practice to receive those services. This is preferable to the “patient attribution” systems currently used by Medicare and health insurance plans to determine when a physician practice should receive a monthly payment for a patient.53 This also allows multiple practices to be involved in delivering different aspects of a patient’s care.
Payments for Patients With Greater Needs
There are at least three types of patients for whom the monthly Condition Management Payments will need to be higher because the physician practice will need to spend significantly more time delivering services to the patients:
- Patients Receiving Initial Treatment for a Chronic Condition. A physician practice will need to spend a significant amount of time with a patient who has been newly diagnosed with a chronic condition in order to provide education and assistance to the patient in implementing the care plan developed for the condition and to make any revisions to the care plan based on (1) any problems the patient experiences in implementing the care plan, and (2) whether the care succeeds in improving the patient’s health. A higher Initial Condition Management Payment will be needed during at least the first month of care in order to support this additional time. For some chronic conditions, and for patients with complex needs, the Initial Condition Management Payment may need to continue for several months to allow adequate time for the care plan to be fully implemented (e.g., if dosages need to be phased in), to assess the efficacy of the treatment(s), to identify any adverse side effects, and, if necessary, to make modifications to the care plan and test their feasibility and effectiveness. When a care plan has been established that is expected to continue for an extended period of time and there is no longer a need for transitional assistance to the patient in implementing it, Initial Condition Management Payments can end and the practice can then begin receiving the standard monthly Condition Management Payments appropriate for the patient.
- Patients With Comorbidities or Barriers to Care. Some patients have a combination of health conditions or have other characteristics (often referred to as “social determinants of health”) that make the patient more susceptible to serious exacerbations or complications. Significantly different or more intensive approaches may be needed for preventing and responding to disease exacerbations and complications of treatment for these patients. A higher monthly Condition Management Payment for a Complex Patient will be needed to enable adequate time to be spent in providing the more intensive level of care management and assistance these patients require. Patients should not be considered to have a complex condition simply because they have multiple chronic diseases; many patients have comorbidities that a physician practice routinely manages in a coordinated way. For example, a high percentage of patients with diabetes also have hypertension and/or hyperlipidemia; the appropriate treatment for patients with diabetes includes management of hypertension and hyperlipidemia, so a patient who has two or more of these conditions should not be classified as having a complex condition solely on that basis. On the other hand, a patient who has no chronic diseases other than diabetes, but who has other characteristics that make standard approaches to treatment and management of diabetes very difficult or impossible (e.g., poverty, blindness, deafness, paralysis, homelessness, illiteracy, etc.) will require significantly more time and assistance, so such a patient would generally be appropriate for this “complex patient” category even though they only have one chronic disease. A patient who has two chronic diseases that co-occur less frequently and where the standard approaches to treating each disease can be in conflict would also be appropriate for this category.54 This is true even if the physician practice is only directly responsible for care of one of the diseases, because of the extra time needed to coordinate services delivered by the practice(s) managing the other disease(s). Because of the diversity of factors that can make delivery of care more difficult, it is not feasible to establish a fixed set of eligibility rules for this category; instead the physician managing the patient’s condition would need to make the determination as to whether an individual patient was appropriate for this category and document the basis for that determination. (Patients with an advanced illness can also be included in this category, but ideally, they should receive comprehensive, multi-disciplinary palliative care services, either from the primary care practice or a palliative care provider, that are supported by payments specifically designed for palliative care.)
- Patients Receiving Complex Treatment Regimens. Some patients will need to receive medications that can have dangerous side effects, multiple treatments that must be carefully sequenced or timed, or treatments that are difficult to use correctly. The staff of the physician practice will need to spend significantly more time assisting these patients, and a higher monthly Condition Management Payment for Complex Treatment will be needed to support this time. As with patient complexity, a variety of factors can contribute to making a particular patient’s treatment more complex, and some patients will find the same treatment regimen more difficult to adhere to than others. Consequently, the physician managing the patient’s condition should be able to make the determination as to whether the treatment regimen for an individual patient is appropriate for this category and document the basis for that determination.
Billing and Paying for Condition Management
Higher payments for the types of patients described above can be easily operationalized by creating separate billing codes for each type of patient, as shown in Figure 13.
FIGURE 13
Monthly Payments for Chronic Condition Management
| CPT/HCPCS Code | Phase of Care | Patient Complexity | Treatment Regimen Complexity | Time Period |
|---|---|---|---|---|
| XX030 | Initial Condition Management | 1-3 Months | ||
| XX031 | Condition Management | Monthly | ||
| XX032 | Condition Management | Complex | Monthly | |
| XX034 | Initial Condition Management | Complex | 1-3 Months | |
| XX035 | Condition Management | Complex | Monthly | |
| XX036 | Condition Management | Complex | Complex | Monthly |
Each of these categories would be assigned either a CPT® (Current Procedural Terminology) code by the American Medical Association’s CPT Editorial Panel or a HCPCS (Healthcare Common Procedure Coding System) Level II code by the Centers for Medicare and Medicaid Services (CMS) HCPCS Workgroup. The physician who is overseeing the patient’s treatment and management would choose the appropriate CPT/HCPCS code based on the phase of care, the complexity of the patient, and the complexity of treatment.
Only one of these codes would be billed for an individual patient in any given month. A different code could be used during a month if the patient’s needs changed during that month (e.g., the patient developed a new problem that made care of the chronic condition more complex or the patient’s treatment had to be changed to a more complex regimen).
If a physician practice bills for one of the Condition Management Payment codes for a patient during a month, it would not bill for evaluation and management services (E/M) fees for any visits that patient makes related to that chronic condition during that month. If the practice bills for a monthly payment, it should be expected to see the patient as often as needed during the month in order to provide good care for the chronic condition. (If the physician practice sees the patient for a different reason, then it could bill for an office visit for that.)
Only one physician practice could bill for one of these codes for the same chronic condition during a single month, but if a patient had two different chronic conditions that were being managed by two different specialists, each specialist could receive a monthly payment for managing one of the conditions.
This approach is both simpler and more effective than the approach to “risk adjusting” payments typically used by Medicare and health insurance plans. In most current risk-adjusted capitation and care management payments, Medicare or the health plan assigns a “risk score” to the patient and adjusts the monthly payment in proportion to that risk score. This approach is problematic, however, because risk scores are generally based only on the types of chronic conditions the patient is diagnosed with, not on other characteristics that may make the patient more complex in terms of chronic condition management, and there are no adjustments for the complexity of the treatment regimen nor for patients who are receiving treatment for the first time. Moreover, this risk adjustment approach cannot be implemented directly in the standard billing and claims payment systems currently used by physician practices and health insurance plans, because the health plan has to calculate the risk score for each patient and multiply that by a default fee in order to determine the actual payment amount, and this means that the physician practice cannot determine in advance what the payment will be.
Accountability for Quality and Utilization
Flexible, monthly Condition Management Payments with higher payment amounts for patients with greater needs enable a specialty practice to deliver proactive, team-based care to a patient with a chronic condition, but they do not assure that the patient will receive appropriate or high-quality care. Consequently, a patient-centered payment system also needs effective mechanisms for ensuring that each patient receives the most appropriate services for their specific condition, that the patient does not receive inappropriate or unnecessary services, and that services are delivered in the most effective way possible.
Problems with Current Approaches
As discussed in Section 2, a number of different “value-based” payment systems have been created to encourage or require high-quality care and reduce unnecessary services, but these approaches have been ineffective in improving the overall quality of care for patients with chronic conditions, they are administratively burdensome, and they can make it more difficult for patients with complex and difficult-to-manage conditions to obtain the type of care they need.
In addition, in an effort to prevent physician practices from ordering or delivering unnecessary and unnecessarily-expensive services, many health insurance companies require a physician to obtain “prior authorization” from the insurance company before the company will pay for certain kinds of medications, tests, or procedures ordered or delivered by the physician. These prior authorization processes are extremely problematic55 for several reasons:
- If there is no clear evidence to guide the physician’s decision about which services to use, there is also no clear evidence to guide the health insurance company’s decision, and the insurance company has far less information about the patient’s symptoms, history, and characteristics to inform its decision than the physician does. As a result, there will still be variation in what services are delivered, but the variation will be driven by differences in the prior authorization rules and decisions made by different health plans and different health plan employees, rather than differences in patient needs.
- Seeking prior authorizations from health plans and challenging inappropriate denials by the health plans requires the physician practice to spend a large amount of time and money56 that does nothing to improve patient care. It also requires the health plan to spend money on staff to review and decide on prior authorization requests. There is no evidence that the savings, if any, from reductions in unnecessary services exceeds the costs incurred by both payers and physician practices to carry out these processes.
- Most prior authorization requests are ultimately approved, so the process merely delays the delivery of care the patients would have received anyway. In some cases, these delays can lead to bad outcomes for patients.
Clearly, a better, more patient-centered approach is needed to ensure high-quality care and to reduce utilization of unnecessary services.
Ensuring Patients Receive Appropriate, Evidence-Based Care
The best way to ensure that each patient receives appropriate services is for the physician practice receiving the Condition Management Payment to deliver services consistent with an evidence-based Clinical Practice Guideline (CPG) or a Clinical Pathway:
- As discussed in Section 3.D, each patient who is diagnosed with a chronic condition should have a written care plan designed specifically for that patient based on the recommendations in an evidence-based Clinical Practice Guideline or Pathway. Since health plan prior authorization programs are supposed to authorize or deny services based on evidence about the effectiveness of the service rather than its cost, there would be no need for a health plan to review and approve a service that was selected based on evidence-based guidelines.
- When the patient begins treatment, they should receive the services specified in that care plan. If the services are ineffective in controlling the patient’s symptoms or preventing exacerbations of the disease, if the treatments have problematic side effects for the patient, or if the patient is unable or unwilling to use the treatments or implement the necessary lifestyle modifications recommended by the CPG, then the physician practice will need to modify the care plan. Modifications should be based on both the evidence and on what services are feasible and effective for the individual patient. These kinds of changes are most likely to occur during the initial treatment phase of care, but could also occur after a care plan has been working successfully for a period of time if the patient’s characteristics or needs change. If the physician makes the changes after consulting current evidence-based guidelines, there would be no need for prior authorization from a health plan.
- If a new treatment is developed that is more effective than the treatment the patient is currently receiving, or if new evidence becomes available regarding the effectiveness of the services a patient is currently receiving, the physician practice should use a shared decision-making process with the patient to determine whether changes should be made to the patient’s care plan. This can occur at any time.
Requiring that the physician practice utilize evidence-based guidelines in implementing a care plan in order to receive Condition Management Payments is a far more efficient and effective way to ensure that patients receive appropriate services than either current quality measurement systems or utilization control programs such as prior authorization:
- Quality measures generally focus only on one or two services or outcomes that the “average” patient is expected to receive or achieve, not the full range of services that are appropriate for an individual patient or the services or outcomes that are most feasible and appropriate for patients with more complex needs. Moreover, there is generally no mechanism for adjusting the quality measure calculation to reflect the subset of patients who need different services when standard therapies are ineffective or cause problematic side effects.
- Since prior authorization, step therapy, and similar requirements focus solely on reducing the use of expensive treatments, they do nothing to ensure that patients who need specific treatments are receiving them.
Operationalizing a requirement to use evidence-based guidelines can be done by requiring the physician practice to attest to two things in order to bill a payer for one of the monthly Condition Management payments listed in Figure 13:
- The physician practice would attest that the patient for whom the bill is being submitted has a written care plan that was developed using the most current Clinical Practice Guideline or Pathway; if the care plan deviates from the recommendations in those guidelines, the physician would attest that the deviation was necessary and the reasons for the deviation are documented in the patient’s clinical record.
- The practice would attest that the patient received all of the services specified in the care plan during the month, unless the patient was unable or unwilling to use the services and the circumstances are documented in the patient’s clinical record.
This is the same approach that is used in current fee-for-service payment systems to assure that a physician practice has delivered the service that it is billing for. For example, when the physician practice submits a bill for an office visit, it is attesting that it had the visit with the patient and that the physician spent either a minimum amount of time in conjunction with the visit or that the decision-making in the visit involved a minimum level of complexity. The practice does not have to submit any documentation to the health plan to prove that a visit occurred or that a specific amount of time was spent, but it maintains documentation in the clinical record that can be used, if necessary, to show that the billing was done properly.
Assessing Patient Needs and Outcomes
Although following the written care plan ensures that all planned treatments and other services are delivered to the patient each month, the physician practice also needs to ensure that the patient receives appropriate services when problems arise and that the services delivered address those problems. This requires that the physician practice proactively monitor the patient’s condition to identify problems and follow up with the patient to assess the outcomes of the services delivered.
Consequently, in addition to using an evidence-based Clinical Practice Guideline or Pathway to develop and modify Care Plans, the physician practice needs to use a Standardized Assessment, Information, and Networking Technology (SAINT) to help it monitor the patient’s chronic conditions. A SAINT provides a systematic way for a patient to provide the physician practice with actionable information about any physical and emotional problems the patient is having and whether the services the practice is providing to the patient are addressing the issues that are of most concern to the patient.57
A successful SAINT will have the following characteristics:58
- Easy to Use and Affordable for the Physician Practice. The SAINT must allow the physician practice to both collect and access information about patients’ needs in a way that does not require a large amount of time by the physician and other practice staff and does not require a significant upfront or ongoing cost in terms of equipment and software.
- Provides Timely, Actionable Information to Guide Care. The information provided by the SAINT needs to tell the practice whether the patient has a problem now, rather than what problems may have existed in the past, and the information needs to be specific enough to allow the practice to determine what initial action to take in response.
- Enables and Encourages Patient Participation. Ideally, the physician practice would receive information from all of the patients in the practice on a regular basis. Because the information describes problems and priorities from the patients’ perspective, patients have to be both willing and able to provide the information to the physician practice. This not only means the SAINT has to be easy for patients to use, but patients need to feel that submitting the information will actually result in better care, and they must not be concerned that the information will be inappropriately shared or misused in any way.59
How’s Your Health is a SAINT that meets all of these criteria:
- It operates through a web-based platform (www.HowsYourHealth.org) that is free for physician practices and easy for patients to use.
- It generates a summary measure called the What Matters Index (WMI) that identifies which patients are experiencing problems and assesses key patient outcomes.60 The WMI has been shown to predict health care spending as well or better than other commonly-used risk stratification/prediction tools.61
- It enables patients to identify specific risk factors, concerns about their health, and problems they have had getting appropriate help so the physician practice can better plan how to assist them.62
- The detailed information submitted by the patient can remain confidential and the patient can decide what information to share with the physician practice or other healthcare providers.
Although How’s Your Health was designed for primary care practices, it can also be used by a specialty care practice to manage patients with chronic diseases. How’s Your Health provides information similar to other methods of surveying patient-reported outcomes, but in a more cost-effective way. It also provides more immediate information about the patient’s experience of care more cost-effectively than the Consumer Assessment of Healthcare Providers and Systems (CAHPS) survey currently used to assess patient experience63 and it avoids the problems associated with patient “satisfaction” ratings.64
Tying Payments to Outcomes
Most patients will achieve good outcomes if their physician practice delivers services consistent with evidence-based Clinical Practice Guidelines. However, for patients with unique needs, there may be no clear evidence as to what should be done, or the evidence-based treatment may turn out to be ineffective or problematic for the patient. In addition, proactive outreach and care management services can be delivered in multiple ways, and even if a specialty practice is delivering these services to patients, it may not be delivering them in the most effective way. Using a SAINT to assess how patients are doing will enable the physician practice to identify when current approaches to services are not working, but it does not assure that the practice will actually use the information to identify problems in care delivery and make improvements.
For many chronic diseases, the clearest signal that a patient may be receiving the wrong treatments or that care management services are not being delivered effectively to the patient is if the patient has to be hospitalized for an exacerbation or complication of their chronic condition. It is impossible for any physician practice to prevent all such hospitalizations, partly because it is impossible to prevent all exacerbations and complications, and partly because the need for hospitalization will depend on what the patient does or does not do when an exacerbation occurs. However, if the patients at a particular physician practice have a significantly higher rate of hospitalizations than similar patients at other practices, it is reasonable to believe that the practice is not delivering treatment and care management services as effectively as possible.
Some value-based payment systems attempt to encourage improved performance by increasing or decreasing all of the payments to the physician practice based on the overall rate of hospitalizations for patients in the practice.65 However, this approach is problematic for several reasons:
- The hospitalization measure often includes all hospitalizations for any reason, not just those related to the chronic condition that the physician practice is managing, which means the practice can be penalized if its patients have other health problems that require hospital treatment.
- Although exacerbations are more likely among some patients with a chronic disease than others, the hospitalization rates are typically not adjusted for all of these differences among patients. As a result, one physician practice may have a higher hospitalization rate than other practices because of differences in the patients it is caring for, not because it is delivering care less effectively.
- The bonuses and penalties are based on hospitalization rates in a prior year, so a practice that is delivering poor-quality care today could actually be paid more than other practices (assuming it had performed better in the past), and vice versa.
- The amount paid for services to an individual patient is based on the average hospitalization rate for all patients, not based on the care the individual patient received. As a result, an individual patient (and their payer) will have to pay for services even if they had to be hospitalized because their care failed to address their needs, and they may even have to pay more for those services if most other patients were able to avoid being hospitalized and the practice qualified for higher payments based on that performance.
- The increase in payment based on good performance may be too small to pay for the additional services the practice must deliver or the different approach to service delivery it needs to use in order to achieve good outcomes for higher-need patients.
A patient-centered approach to outcome-based payment should be structured very differently:
- There should be no payment for ongoing chronic condition management during a month in which hospitalization occurs. Following the initial months of treatment, the physician practice should not bill for a Condition Management Payment for a patient during a month in which the patient was hospitalized for an exacerbation of the chronic condition or a complication of treatment for that condition. This is not a “penalty” per se, but rather a reflection of the fact that much of the patient’s care during that month was provided by the hospital, not the physician practice. This should not apply to the Initial Condition Management Payments, however, since a new patient could experience disease exacerbations requiring hospitalization until the physician practice is able to find a treatment and care plan that will work effectively for the patient.
- Monthly Condition Management Payments should be set at levels that will generate sufficient revenue during the year to cover the expected cost of effective care, assuming that some hospitalizations will occur no matter what the physician practice does. In the payment categories in Figure 13, the payment amounts in the categories for patients with higher needs and patients receiving more complex treatments would be higher both because the patient will need more proactive services and because the risk of hospitalization will be higher.
Quality Assurance in Patient-Centered Payment vs. Current Payment Systems
In summary, under Patient-Centered Payment for Care of Chronic Conditions, the physician practice would only be able to bill for and be paid for a monthly Condition Management Payment if three criteria were met:
- The practice had delivered (or ordered) all of the services during the month that were recommended for the patient by an appropriate Clinical Practice Guideline or Pathway, and it did not deliver or order any services that were not recommended by such guidelines, unless there was a patient-specific justification for deviating from the guidelines that was documented in the patient’s clinical record.
- The practice used a SAINT to monitor the patient’s health in order to identify any problems the patient was having and to provide appropriate services in response.
- The patient was not hospitalized during the month for an exacerbation of their chronic disease or for a complication of the treatment they were receiving for the disease.
If any one of those criteria is not met for a particular patient during the month, the physician practice would not receive a Condition Management Payment for that patient for that month.
This is a much higher standard of quality than exists under the current fee-for-service system or any current value-based payment system. Under current payment systems, the practice would be paid for an office visit or for care management services even if:
- the patient failed to receive all of the services recommended by evidence and there was no documented justification for this;
- the patient received unnecessary or unnecessarily-expensive services;
- the practice did nothing to proactively monitor the status of the patient’s health; and/or
- the patient was hospitalized for an exacerbation of their disease or a complication associated with their treatment.
This also provides much greater assurance of quality than existing approaches to quality measurement and performance-based payment. Current quality measures assess only specific types of services for specific types of patients, whereas Clinical Practice Guidelines have much broader standards as to what services are appropriate and necessary. Moreover, under current performance-based payment systems, a patient or their insurance plan still pays for services to a patient even if those services did not meet the standards specified in quality measures, whereas under Patient-Centered Payment, there would be no payment for the patient unless evidence-based services were delivered to that patient.
FIGURE 14
Quality Assurance Under Current Payment Systems and Patient-Centered Payment
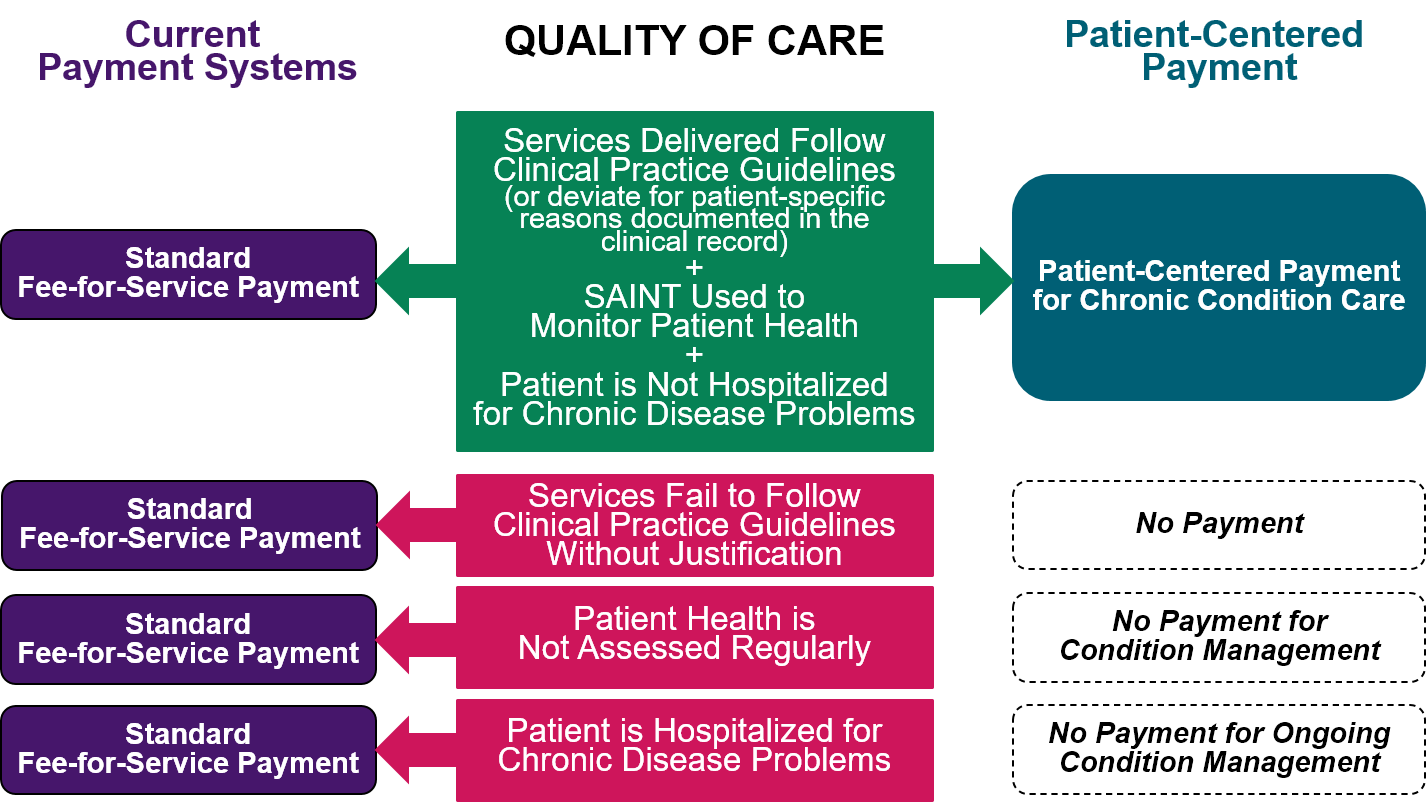
Improving Clinical Practice Guidelines
Using evidence-based guidelines for condition management will result in better outcomes for patients as long as there is evidence available as to what services will improve outcomes for the patients. As with diagnosis, evidence developed through small, controlled studies with selected patients may not apply to more diverse patient populations, and if there is little or no evidence available, a guideline may not exist or the guideline may not be appropriate for a specific patient. In these cases, physicians will need to deviate from the guidelines. However, the outcomes of treatment and management in these cases should ideally be analyzed in order to better guide decisions in the future.
As discussed in Section 3.C.2 in conjunction with diagnosis, a Standardized Clinical Assessment and Management Plan (SCAMP) is a form of Clinical Practice Guideline/Pathway that is explicitly designed to allow deviations from guidelines in appropriate situations and to use information about the circumstances and reasons for deviations and the outcomes of those choices in order to improve the guidelines.66
The outcome information derived from the SAINT will support this approach. Portions of the outcome information provided by the patient should be combined with information in the patient’s clinical record and submitted to a Clinical Data Registry (CDR) so that it can be analyzed and used to improve evidence-based guidelines. As described in more detail in Section 3.C, a CDR is a database that assembles information from multiple physician practices in a way that supports analysis and research on the effectiveness of different approaches to diagnosis and treatment for patients with specific characteristics.
Since creating and maintaining registries is an expensive endeavor both for the specialty societies that manage them and for the physician practices that submit data to them, in order to support a true SCAMP process, the Condition Management Payments need to be large enough to enable specialists to participate in CDRs and to spend the time needed to document not only the reasons for deviations from guidelines, but also the outcomes for the patients.
Adequacy of Payment
Challenges in Determining Adequate Payment Amounts
The amounts of the Condition Management Payments have to be sufficient to cover the time and cost involved for both the physician and other practice staff to provide high-quality services and support to patients in each of the categories of Condition Management Payments described in Figure 13. Many of the most important aspects of care for a chronic condition are not delivered in office visits with physicians, particularly the support provided to patients by nurses and other practice staff who cannot directly bill for services and whose time is not currently counted in determining which fee can be billed. Unfortunately, there is very little published research available on how much time is currently spent on these activities, how much time is needed to provide high-quality care for a patient with a chronic disease, and how much more time is needed for patients who have a complex condition or are receiving a complex treatment regimen.
It will likely be impossible to know exactly how much time is required to carry out these tasks until payments are adequate to support performing them. As with the Diagnosis Payments and Care Planning Payments, the only way to resolve this “chicken and egg” problem will be to begin using Condition Management Payments with payment amounts based on best estimates of time and costs (accepting the reality that those amounts may not be exactly right), allow specialty practices to use the payments to deliver high-quality care management services, gather data on how much time is actually needed to do this, and then refine the payment amounts over time as those data become available.
Time Needed for Care of Established Patients With Non-Complex Conditions
The only published estimate of the time required for care of patients with chronic conditions was based on the amount of time that a primary care physician would need to spend in order to follow clinical guidelines for care of such patients.67 The study estimated that a physician with a typical primary care patient panel (2,500 patients) would need to spend 2,484 hours per year on chronic disease care for the subset of patients who had one or more chronic conditions.68 Assuming that 45% of the patients in the total patient panel had at least one chronic condition69 (i.e., 1,125 patients), this translates into an average of 2.2 hours per chronic condition patient per year (the equivalent of about six 20-minute visits).
Another study estimated that 25-47% of this time could be delegated to a nurse (or other non-clinician staff member).70 If one assumes that a nurse is available and that 40% of the required time is delegated to the nurse, the physician would spend a total of about 72 minutes per year per patient, and the nurse would spend about 48 minutes per year.
These estimates are likely too low for truly patient-centered chronic care, for the following reasons:
- Additional time would be needed for the physician to consult, apply, and document the use of Clinical Practice Guidelines for each patient and to communicate with the patient’s primary care physician. It seems reasonable to assume that the physician would need to spend at least 10-15 minutes each year on these tasks for each patient with a chronic condition.
- Since the estimates were based on what the physician would be expected to do in office visits and what portion of those tasks could be delegated to a nurse, the estimates did not include any provision for additional time that should be spent by a nurse or other member of the practice staff in (1) proactively contacting patients to monitor their symptoms, or (2) responding to calls from patients between visits to ask about worrisome symptoms, how to use medications, etc. It seems reasonable to assume that the nurse or other staff would need to spend an average of at least an additional hour per patient per year to perform these tasks.
In combination, these estimates imply that providing quality care for a group of patients with a chronic condition would require the physician, nurse, and other practice staff to spend an average of at least 3.5 hours per patient per year, or about 17 minutes per patient per month. This average amount is not intended to represent the amount of time needed for each individual patient; some patients will need more time than this, while others will need less. The amount of time an individual patient needs may vary from year to year as well as from month to month.
This estimate of average time is consistent with the amount of time that the staff of a diabetes clinic at an academic medical center reported spending to care for patients with diabetes.71 Physicians and nurse practitioners spent an average of about 1.2 hours per patient per year, and nurses and other clinic staff spent about 2 hours per patient per year, for a total of 3.2 hours per patient per year. The study noted that there was no payment for the time spent by the nurses and other clinic staff helping patients in between physician visits.
Time Needed for Care of Established Patients With Complex Conditions
Patients with complex conditions and those receiving complex treatments will require more time from both the physicians and from the nurses and other care management staff. However, there are no data available on how much time is needed to provide effective chronic condition management services to such patients, so assumptions will need to be made about the additional time needed.
Time Needed for Physician Services
Current Medicare payments for office visits with established patients are 40% higher if more complex medical decision-making is required, and the payment is twice as high for a visit requiring high-complexity decision-making than for a visit with low-complexity decision making.72 Assuming similar ratios apply to the differences in the average monthly time spent by physicians in providing condition management services to patients, one can estimate that the physician would spend about 2 hours per year for patients with a complex condition or complex treatment, and about 3 hours per year for patients with both a complex condition and complex treatment.
Additional time would be needed for the physician to consult, apply, and document the use of a Clinical Practice Guideline or Pathway for each patient and to communicate with the patient’s primary care physician and any other specialists involved with the patient’s care. It seems reasonable to assume that the physician would need more time to do this for a complex patient than for a non-complex patient, e.g., at least 5 minutes more per month.
Time Needed from Other Practice Staff
Currently, Medicare will pay an additional fee to a physician practice if a nurse or other member of the practice staff spends the following amounts of time during a month providing care management services to the following types of patients:
- 30 minutes for a patient with one “complex chronic condition expected to last at least 3 months and that places the patient at significant risk of hospitalization, acute exacerbation/decompensation, functional decline or death.” The condition must require “frequent adjustments in the medication regimen” and/or the “management of the condition is unusually complex due to comorbidities.” (CMS refers to this as “Principal Care Management.”)73
- 20 minutes of time for a patient with “multiple (two or more) chronic conditions expected to last at least 12 months, or until the death of the patient.” The conditions must “place the patient at significant risk of death, acute exacerbation/decompensation, or functional decline.” Although CMS describes this as “Non-Complex” Chronic Care Management, many of the patients defined earlier as having a “complex condition” would meet the CMS eligibility criteria. Medicare pays an even higher fee if at least 40 minutes of time is spent.74
- 60 minutes of time for a patient with “multiple (two or more) chronic conditions expected to last at least 12 months, or until the death of the patient” that “place the patient at significant risk of death, acute exacerbation/decompensation, or functional decline,” if “moderate or high complexity medical decision making” is required. (CMS refers to this as “Complex Chronic Care Management.”)75
CMS has not provided any rationale for the minimum times of 20 minutes and 30 minutes of care management services the practice staff must deliver during the month in order to be paid for the services, nor has it provided any rationale as to why less time is required for management of patients with two chronic diseases than those who have one disease.76 When CMS first proposed a fee for chronic care management services to patients with two or more conditions, it planned to make one payment for a three-month (90 day) period, and non-physician staff would have been required to provide a minimum of 60 minutes of services to the patient over the course of the three months.77 However, CMS decided to modify the proposal and pay separate fees for each month of care management rather than a single fee for three months. When this was done, the 60-minute minimum for three months was converted into a minimum of 20 minutes each month.78 Requiring a minimum of 20 minutes each month is far more restrictive than requiring a minimum of 60 minutes every 90 days. For example, if the staff in a physician practice spend 25 minutes on care management for a patient each month for two months and 10 minutes in the third month, the practice would only qualify for fees in the first two months, even though 60 minutes in total was spent over the course of 90 days. Spending 30 minutes each month for two months would only qualify for the one payment each month, but spending 40 minutes one month and 20 minutes the next month would qualify for an additional payment for the extra 20 minutes in the first month, even though the total time spent is the same over the two-month period. This creates a perverse incentive for the practice staff to spend more time with a patient than is actually necessary in order to qualify for payment, or even to delay spending all of the extra time a patient needs until a subsequent month in order to qualify for payment in that month.
A more patient-centered approach would be to use 30 minutes per month as an estimate of the average time needed per month to provide care management for patients with a complex condition or complex treatment, to provide a payment each month that is adequate to support that amount of time on average, and to require that the patient receive the care management services they need without requiring any specific amount of time be spent on that during the month. Since patients with both a complex condition and complex treatment will need more time than patients with only one of those characteristics, it could be assumed that an average of 40 minutes per month would be needed for them.
Total Time for Established Patients With Complex Conditions
Figure 15 shows these estimated times for patients with complex chronic conditions and/or complex treatments as well as the estimated times for patients with non-complex conditions discussed earlier. The combination of physician and nursing time would average 45 minutes per month for a patient who has either a complex condition or who receives a complex treatment regimen – which is about three times as much as for patients with non-complex conditions – and 60 minutes per month for the patients with both complex conditions and complex treatments.
FIGURE 15
Estimated Time Needed to Deliver Ongoing Condition Management Services
| Phase of Care | Patient Complexity | Treatment Regimen Complexity | Physician Time with Patient (Minutes) | Nurse Time with Patient (Minutes) | Physician Documentation & Coordination with Primary Care (Minutes) | Average Total Time Per Month (Minutes) |
|---|---|---|---|---|---|---|
| (Ongoing) Condition Management | Non-Complex | 7 | 9 | 1 | 17 | |
| (Ongoing) Condition Management | Complex | 10 | 30 | 5 | 45 | |
| (Ongoing) Condition Management | Complex | 10 | 30 | 5 | 45 | |
| (Ongoing) Condition Management | Complex | Complex | 15 | 40 | 5 | 60 |
Time Needed for Initial Management of Patients With Chronic Conditions
The time estimates above represent the time required for ongoing management of the patient’s condition after a feasible and effective treatment and care plan has been identified. As discussed earlier, much more time will generally be needed during the initial month of treatment, or even the first several months of treatment, than in later months because of the need to (1) provide patients with education about their condition, about the treatment they will be receiving, and about the steps they need to take in self-management, and (2) to monitor and make adjustments to the initial care plan based on whether it is feasible for the patient to adhere to it and whether it is effective in controlling the patient’s condition. Patients who are receiving a complex treatment regimen will likely require an even higher amount of time.
Time Needed for Physician Services
It is reasonable to expect that the patient’s physician would see them at least once during the month after treatment begins. An office visit during this period would likely qualify as at least “moderate complexity” and therefore require at least 30 minutes of the physician’s time (i.e., a Level 4 Evaluation & Management Services visit). A visit with a patient receiving a complex treatment regimen would likely qualify as “high complexity” and require 45 minutes of time, i.e., 50% more. If the initial treatment period needs to extend longer than a month, then it could similarly be assumed that the physician would see the patient once during each of those months, either in person or through a telehealth visit.
Additional time would be needed for the physician to consult, apply, and document the use of Clinical Practice Guidelines for each patient and to communicate with the patient’s primary care physician and any other specialists involved with the patient’s care. This will likely take a significant amount of time during the initial month of treatment, particularly if adjustments are being made in treatment and care management services, so it seems reasonable to assume that the physician would spend at least 10 minutes during the month on these tasks in addition to the time spent with the patient.
Time Needed from Other Practice Staff
During the initial month(s), the nurse or other practice staff should be providing the patient with extensive education about their condition, about the treatment(s) they are receiving, and about self-management approaches. As a result, far more time will need to be spent with the patient than in later months. If the nurse spends an average of 15 minutes per week with the patient, that would total 60 minutes for the month. If one assumes that a patient with a complex treatment regimen requires 50% more time, that would represent 90 minutes for the month.
Total Time for Patients Receiving Initial Condition Management
Figure 16 shows these estimated times for patients during the initial month of treatment (or the initial months, if more than one month is needed). The combination of physician and nursing time would total 100 minutes (i.e., one hour and 40 minutes) during the month, and 145 minutes (i.e., two hours and 25 minutes) for a patient who is beginning a complex treatment regimen.
FIGURE 16
Estimated Time Needed to Deliver Initial Condition Management Services
| Phase of Care | Treatment Regimen Complexity | Physician Time with Patient (Minutes) | Nurse Time with Patient (Minutes) | Physician Documentation & Coordination with Primary Care (Minutes) | Average Total Time Per Month (Minutes) |
|---|---|---|---|---|---|
| Initial Condition Management | 30 | 60 | 10 | 100 | |
| Initial Condition Management | Complex | 45 | 90 | 10 | 145 |
Cost of Delivering Condition Management Services
Figure 17 summarizes the estimated times that would be spent by physicians and other practice staff providing condition management services for patients in each of the categories in Figure 13.
FIGURE 17
Estimated Time Needed to Deliver Condition Management Services
| Phase of Care | Patient Complexity | Treatment Regimen Complexity | Physician Time with Patient (Minutes) | Nurse Time with Patient (Minutes) | Physician Documentation & Coordination with Primary Care (Minutes) | Average Total Time Per Month (Minutes) |
|---|---|---|---|---|---|---|
| Initial Condition Management | 30 | 60 | 10 | 100 | ||
| (Ongoing) Condition Management | 7 | 9 | 1 | 17 | ||
| (Ongoing) Condition Management | Complex | 10 | 30 | 5 | 45 | |
| Initial Condition Management | Complex | 45 | 90 | 10 | 145 | |
| (Ongoing) Condition Management | Complex | 10 | 30 | 5 | 45 | |
| (Ongoing) Condition Management | Complex | Complex | 15 | 40 | 5 | 60 |
Estimates of the dollar cost associated with the time spent by physicians and by nurses were developed in Section 4.C.3 and Section 4.D.3 in conjunction with Diagnosis Payments and Care Planning Payments. These can be used to translate the estimated times in Figure 17 into estimates of the amounts needed for the Condition Management Payments. Although many aspects of care management services can be provided by staff other than a nurse (e.g., diabetes educators, social workers, pharmacists, behavioral health specialists, and medical assistants), small practices will not have enough patients to support teams with more specialized skills. Payments that are adequate to support time spent by a nurse will generally also be adequate to support a staff with more diverse skills, but the reverse may not be true. Consequently, the cost and payment estimates here will be based on the costs of employing a nurse to carry out tasks that are not performed by the physician. (Section 3.H.3 shows how the payments could support different types of staff in a larger practice.)
Many patients with a stable chronic condition could have their treatment and care directed by a nurse practitioner rather than a physician, which would result in a lower hourly cost for the clinical component of the time involved in these patients’ care. However, a small specialty practice, such as a practice in a rural area, may not have enough patients to require the time of two clinicians, particularly if the practice has one or more nurses and the physician can delegate an appropriate portion of their care management tasks to the nurse. Payments that are adequate to support a practice with two physicians will also be adequate to support a practice with a physician and a nurse practitioner, but the reverse is not true. As a result, the cost and payment estimates here will assume that all care that cannot be delegated to a nurse will be performed by a physician. (Section 3.H.3 shows how the payments could support different types of clinicians in a larger practice.)
Based on these assumptions, Figure 18 shows estimated amounts for Condition Management Payments determined by multiplying the time estimates in Figure 17 by the hourly costs for physicians and nurses and adding a small (3%) margin. As noted earlier, if the specialist earns a higher annual salary, then the hourly cost of the practice would be higher and the payment amounts would need to be correspondingly higher.
FIGURE 18
Estimated Time and Payment Amounts for Condition Management Services
| Condition Management | Patient Complexity | Treatment Regimen Complexity | Total Physician Time (Hours) | Cost of Physician Time (Per Hour) | Total Nurse Time (Hours) | Cost of Nurse Time (Per Hour) | Estimated Cost of Services Per Month | Margin | Payment Amount Per Month |
|---|---|---|---|---|---|---|---|---|---|
| Initial Condition Management | 0.67 | $211 | 1.00 | $59 | $200 | 3% | $206 | ||
| (Ongoing) Condition Management | 0.13 | $211 | 0.16 | $59 | $36 | 3% | $37 | ||
| (Ongoing) Condition Management | Complex | 0.25 | $211 | 0.50 | $59 | $82 | 3% | $85 | |
| Initial Condition Management | Complex | 0.92 | $211 | 1.50 | $59 | $282 | 3% | $290 | |
| (Ongoing) Condition Management | Complex | 0.25 | $211 | 0.50 | $59 | $82 | 3% | $85 | |
| (Ongoing) Condition Management | Complex | Complex | 0.33 | $211 | 0.67 | $59 | $110 | 3% | $113 |
It is important to recognize that these payment amounts are designed to support all of the “evaluation & management services” the practice provides, including any visits the physician has with the patient (whether an in-person visit in the physician’s office or a telehealth visit) as well as what are traditionally called care management services. A physician practice receiving one of the payments in Figure 18 for a particular patient would not bill that patient or their health insurance plan separately for any individual visits with the patient or for any other specific types of care management services for which separate fees are currently paid.
Adjusting Payments for Expected Hospitalization Rates
As discussed in Section 3.E.2, the physician practice could be held accountable for outcomes by not paying it a Condition Management Payment in a month in which the patient is hospitalized. However, it is highly likely that at least some patients will be hospitalized no matter how good the care they receive from the physician practice. The care should be viewed as successful if it avoids the high rates of hospitalization commonly experienced by patients with chronic conditions, particularly patients with complex conditions, even if it does not prevent all hospitalizations.
Since the payments defined in the preceding section were intended to just cover the practice costs with a small profit margin, failure to receive the payments for a small percentage of patients during a month that they are hospitalized would cause a financial loss for the practice. Consequently, an adjustment must be made to the payments so that the physician practice still receives adequate payment to cover its costs if its patients are hospitalized at the lowest rate likely to be achieved. This can be done simply by dividing the payment calculated in the previous section by the percentage of patient-months in which hospitalizations would be expected not to occur.
For example, Figure 19 shows a hypothetical specialty care practice providing condition management services for an average of 1,400 patients per month. For simplicity, it will be assumed that all of the patients have completed the initial phase of treatment and that none of the patients have complex needs or are receiving complex treatments. The estimated annual cost of providing condition management services to these patients is $621,000 (based on an assumption that one FTE physician and 1.5 FTE nurses would be needed to provide ongoing treatment and care management for these patients).
FIGURE 19
Impact of Hospitalization Rates on
Practice Revenue from Condition Management Payments
| Hospitalization Rate | ||||
|---|---|---|---|---|
| As Expected | As Expected | High | Low | |
| Total Patients Per Month | 1,400 | 1,400 | 1,400 | 1,400 |
| Hospitalization Rate | 5% | 5% | 10% | 1% |
| Condition Management Payment | ||||
| Unadjusted Payment Per Patient | $37 | |||
| Adjusted Payment Per Patient | $40 | $40 | $40 | |
| Annual Condition Management Revenue | $593,000 | $638,400 | $604,800 | $665,280 |
| Annual Condition Management Cost | $621,000 | $621,000 | $621,000 | $621,000 |
| Net Revenue | ($28,000) | $17,400 | ($16,200) | $44,280 |
| % Margin | -4.5% | 2.8% | -2.6% | 7.1% |
If one assumes that even with effective condition management services, 5% of the patients will be hospitalized for an exacerbation of their condition once during the course of the year, then paying $37 per month per patient (the amount calculated in Figure 18) during only 95% of the months would result in a financial loss for the practice. Consequently, the monthly payment would need to be increased to $40 per month in order to generate enough revenue to cover the practice’s cost.
As shown in Figure 19, the higher payment would only cover the practice’s costs if the actual hospitalization rate for the patients in the practice is at or below the expected level. If the patients in the practice are hospitalized at a significantly higher rate (10% instead of 5%), the practice would lose money. There would also be a financial incentive for the practice to take extra steps to help its patients avoid hospitalizations; as shown in Figure 19, reducing the hospitalization rate below the expected level of 5% would result in a higher profit margin for the practice.
Patients with more complex conditions will be more likely to experience circumstances requiring hospitalization, so larger adjustments would be needed to the payments for care of those patients. Figure 20 shows the adjusted amounts assuming that 10% of patients with complex conditions or complex treatments would ordinarily be expected to be hospitalized during the year and that 15% of patients with both complex conditions and complex treatments would be hospitalized.79 No adjustment would be needed to the Initial Condition Management Payments because it would be inappropriate to hold physician practices accountable for patient hospitalization rates during this initial period of time.
FIGURE 20
Condition Management Payments Adjusted for Expected Rates of Hospitalization
| Code | Condition Management | Patient Complexity | Treatment Regimen Complexity | Unadjusted Payment Amount Per Month | Expected % of Patients Admitted to Hospital | Adjusted Payment Amount Per Month |
|---|---|---|---|---|---|---|
| XX030 | Initial Condition Management | $206 | $206 | |||
| XX031 | (Ongoing) Condition Management | $37 | 5% | $40 | ||
| XX032 | (Ongoing) Condition Management | Complex | $85 | 10% | $94 | |
| XX034 | Initial Condition Management | Complex | $290 | $290 | ||
| XX035 | Condition Management | Complex | $85 | 10% | $94 | |
| XX036 | Condition Management | Complex | Complex | $113 | 15% | $133 |
Patient Access and Choice
Choice of Physician Practice
A patient should be able to receive chronic condition management services from the physician practice that is best able to address the patient’s needs. Patients who have severe conditions, uncommon conditions, multiple chronic conditions, patients for whom standard treatments are not effective or have problematic side effects, and patients who face barriers in using standard approaches to care may need specialized expertise or services that only certain physician practices can provide.
In many health insurance plans, patients can only receive full coverage for services if they are delivered by physicians who are part of a payer-defined network, and the network is defined primarily based on whether the physicians will accept discounted fees for traditional services. This can prevent patients from receiving the services that will be most effective for them. Instead, patients should be able to select any physician practice that is willing to accept the patient-centered payment amounts and deliver evidence-based care in return.
Patient Cost Sharing
For patients with insurance, there should ideally be no co-payments or co-insurance for the monthly Condition Management Payments, nor should they be subject to a deductible. The goal of these services is to prevent chronic condition exacerbations from occurring, and since the savings to the payer (i.e., Medicare or a health insurance plan) from not having to pay for hospital treatment of exacerbations will likely exceed the cost of the monthly condition management services, it would be undesirable to create cost barriers that could discourage patients from enrolling to receive these services.
If it is necessary to charge cost-sharing, it would be preferable to charge a small co-payment for the initial month of condition management services, and then no cost-sharing for the rest of the year. This would be more efficient for both the physician practice and the patient than billing and collecting small amounts every month (e.g., 20% co-insurance on the $40 monthly payment would be $8 every month). This approach could also help ensure that only patients who have a chronic disease needing proactive care management would enroll for the services, while encouraging patients to continue receiving the services once they started. If this one-time cost-sharing amount is less than or equal to the cost-sharing that would be charged for an office visit with the physician, then the patient would not have a financial incentive to choose a single office visit with the physician rather than enrolling for ongoing condition management services.
Unfortunately, under federal law, Medicare beneficiaries are required to pay 20% of the cost of any payment for a physician’s service unless the service is specifically classified as a required preventive care service. Paying cost-sharing every month could deter Medicare beneficiaries from enrolling for ongoing condition management services, and a requirement to pay more for higher-intensity services would financially penalize higher-need patients who require more assistance from the physician practice to successfully manage their condition. To avoid this problem, Congress will need to amend the current statute.
Payment for Administration of Medications
For most patients with a chronic disease, their primary treatment will consist of one or more oral medications that the patient will obtain from a community pharmacy. Patients will need education from the physician practice about how and when to take these medications, and some will need advice and/or assistance from the practice regarding what to do if a medication dose is skipped, if circumstances (such as travel) make it difficult to follow the standard schedule, or if problematic side effects arise. The monthly Condition Management Payments described in the previous section enable the physician practice to have sufficient staff available to provide the education patients need and to respond to questions and concerns in a timely fashion.
For some patients, the appropriate medications cannot be taken orally, and they will need to be injected or infused by a physician or a nurse. This procedure has to be performed in person, either in the practice office, in a hospital or other infusion center, or in the patient’s home. If the physician practice performs the procedure, it can bill and be paid for the injection or infusion procedure using fees that are already available. The fees paid by Medicare for these procedures are supposed to be set at levels adequate to cover the time spent by the physician or nurse in performing the procedure and the equipment involved in doing so.
Although current billing codes for the injection or infusion procedure can continue to be used for payment, a different approach is needed to pay for the drugs that are administered. In order to administer drugs to patients, the physician practice has to purchase an inventory of the drugs it expects to be using, and Medicare and health insurance plans pay the practice for the drugs after they are administered to individual patients. This process is commonly referred to as “buy and bill.” It is beneficial for patients because the physician practice can immediately administer needed drugs without waiting for the drugs to be shipped to the patient or the practice from an outside pharmacy, but it requires that the practice pay for the drugs and wait for reimbursement, and it requires the practice to set up and staff an internal pharmacy to acquire, store, and dispense the drugs, as well as to have an adequate number of nurses and other staff to administer the drugs to the patients.
Unfortunately, the methodology used by Medicare and most commercial payers to pay a physician practice for the drugs it has purchased is very problematic. Under the typical approach, which is referred to as “ASP+x%,” the payment the practice receives for a drug is equal to (1) the most recent national figure for the “Average Sales Price” (ASP) of the drug, plus (2) an additional amount equal to a percentage of the ASP amount.80 The x% component is intended to cover the additional expenses that the practice incurs (1) to purchase and store medications, such as the costs of hiring pharmacists and buying medication storage equipment, and (2) to cover the loss in revenue the practice experiences if a medication vial is accidentally broken and cannot be used or if a patient needs less than a full vial of a drug for their treatment.
In many cases, even with the x% add-on, the total amount will be less than what the practice had to pay to obtain the drug from a manufacturer or wholesaler, particularly for small practices that are not eligible for the same quantity discounts and rebates offered to larger practices and health systems. Moreover, the payment amount will almost always be less than the current price of a drug when the price of the drug has increased, since the ASP amount is calculated based on the prices of drugs in sales that occurred two quarters earlier. As a result, in many cases, a physician practice will lose money if it gives patients the medications they need. In other cases, the ASP+x% amount could be significantly higher than the acquisition cost of the drug (for example, if the drug price has recently been reduced, the ASP amount would be based on the earlier, higher price), which means the physician practice would lose money by not administering the drug, even though it may not be the best drug for the patients.81
The potential for large losses and profits on drugs administered in physician practices should be eliminated by replacing the current ASP+x% payment for drugs with a new Practice-Administered Drug Cost (PADC) Payment that has three components:
- Payment for Drug Acquisition Cost. The practice needs to receive a payment equal to the practice’s actual cost of acquiring the drug the patient receives. This would ensure that the physician practice has no financial incentive to avoid using the drug that will work best for the patient. Since the practice would be required to follow a Clinical Practice Guideline or a Clinical Pathway in prescribing medications, the practice would only use a more expensive drug if evidence supported doing so.
- Payment for Wastage/Breakage Losses. An additional payment equal to a small percentage (e.g., 1-2%) of the drug cost is needed to cover the expenses associated with wastage and breakage. Since these costs are proportional to the cost of the drug, this payment component would need to be proportional to the drug cost, but since the percentage would be very small and designed to cover a specific cost the practice could incur, it would not create a financial incentive to use a more expensive drug.
- Payment for the Costs of Pharmacy Operations. An additional fixed monthly payment for each patient enrolled for ongoing condition management is needed in order to cover the costs of operating the practice’s pharmacy. The cost of operating a practice pharmacy will be proportional to the number of patients treated, not the cost of the drugs used, so the payment should be a per-patient payment, not a percentage of drug costs. The amount should be based on (1) the estimated cost of operating a pharmacy in a physician practice and (2) the average number of patients enrolled for condition management in a practice that has enough patients to support the staff and equipment necessary for administration of drugs. The practice should receive this payment for all patients who are enrolled for chronic condition management, not just those receiving infused or injected medications, in order to ensure there is no financial incentive to use infused or injected medications on patients who do not need them.
In addition to changing the method of paying the physician practice for the drugs, physician practices should not be expected to collect large cost-sharing payments for the drug from patients. For example, Medicare will currently only pay the physician practice 80% of the ASP+x% amount; the practice must collect the remaining 20% from the patient unless the patient has supplemental insurance to cover that. If a patient cannot afford to pay that amount, the physician practice can incur a significant financial loss when it administers a very expensive drug. If this type of cost-sharing is required, then the percentage used in the second component of the PADC Payment would need to be increased in order to create a pool of funds at the practice that it can use to cover patient bad debt.
Payment for Practice-Based Testing
If a patient needs basic laboratory tests in order for their physician to monitor their chronic condition or evaluate their medication dosage levels, it would be desirable for the patient to have the ability to obtain those tests at the physician practice rather than having to go to a hospital or separate laboratory, particularly if the patient needs to visit the practice for other reasons.
There are fees currently available for the laboratory tests that physician practices can perform, but some of the fees may not be adequate to cover the costs of the equipment and supplies with the volume of tests that would typically be performed in a small physician practice. Information should be gathered from physician practices to determine the average cost of providing common tests that would be desirable to perform on site, and if those costs are higher than current fees, higher fees for the tests should be paid to practices that are receiving the Condition Management Payments. Because the practice would be following Clinical Practice Guidelines in ordering tests, and because the payments for the tests would be based on the estimated costs of performing the tests, there should not be any concern about the tests being overused if the payments are increased above current levels.
Adequacy of Overall Payment for Practices
A good payment system must ensure that a physician practice or other healthcare provider will receive adequate revenue to support the costs of providing high-quality care to all types of patients, particularly the patients who have the greatest needs. Otherwise, providers will be forced to “cherry pick” the subset of patients for whom payments are adequate, which would limit access for higher-need patients and cause disparities in outcomes.
Practices Caring for Higher-Need Patients
The Problems With Fee-for-Service Payment
In theory, fee-for-service payment can do a good job of adjusting a practice’s revenue based on the needs of its patients, since the practice will receive additional fees when patients with higher needs receive additional services. However, under the current fee-for-service system:
- physician practices are paid primarily based on the number of visits the patient makes, so if the practice can successfully manage a patient’s chronic condition with fewer visits, the practice will lose money.
- the fee for a visit is the same regardless of the purpose of the visit and regardless of whether the practice needs to spend more time before or after the visit because of the complexity of the patient’s needs. Since higher-need patients will require more time before, during, and/or after visits than other patients, a practice that has more high-need patients will not be able to see as many patients in total, and its revenues will be reduced under current visit-based payment systems.
- current fees for chronic care management services require that a specific minimum amount of time be spent providing services to the patient during the month (e.g., Medicare requires that at least 30 minutes be spent on a particular patient’s care during the month in order to bill for a “Principal Care Management” payment). If the practice has to spend more or less time on care of an individual patient during a month, the payment will be less than the cost of the time that is actually spent.
As a result, the fees paid will generally be less than the actual cost of delivering services to higher-need patients.
In addition, prior to the COVID-19 pandemic, physician practices were only paid for a visit if the patient was seen in person in the physician’s office. Although many visits began occurring though video or telephone contacts with patients in their own homes, the law and regulations that authorize this are set to expire after the formal public health emergency associated with the pandemic ends. This will make it more difficult for physician practices to receive adequate payment for caring for patients, particularly higher-need patients.
The Problems With Population-Based Payment
Under population-based payment systems, the practice receives a single monthly payment for each patient (i.e., capitation) instead of fees for individual services. While this provides greater flexibility than service-specific fees, the monthly payment will only be adequate if it is appropriately “risk-adjusted” for differences in patient needs. However:
- typical risk adjustment systems only consider the types of diseases a patient has, and they ignore many other patient characteristics, including “social determinants of health,” that can have equal or bigger impacts on the time and costs incurred by a physician practice.
- standard risk adjustment systems only consider chronic diseases diagnosed in the past, not the patient’s current health problems. For example, even though a physician practice will likely spend more time with a patient during the months just before and after they are diagnosed with a chronic condition than in the following years, standard risk adjustment systems pay in exactly the opposite way – they pay more in the year after the year in which the condition is diagnosed.
As a result, population-based payment systems can penalize physician practices for providing services to many of the highest-need patients.
The Strengths of Patient-Centered Payment
Patient-Centered Payment for Care of Chronic Conditions would do a better job of aligning payments with the cost of caring for individual patients than either the current fee-for-service system or population-based payments, because the payments are designed to match the specific types of services patients need – diagnosis, care planning, and condition management – and to match the amount of time required to deliver those services to different kinds of patients. Under Patient-Centered Payment, the physician practice has the flexibility to deliver services to patients in whatever way works best for the patient – through a face-to-face office visit, a video visit in their own home, or a telephone call. Moreover, a visit or call could be with the physician, nurse, or someone else on the practice team – whomever is best able to help the patient.
In addition, any physician practice must adjust the number of patients it enrolls for care based on the needs of those patients. If a larger percentage of its patients have complex conditions, the practice will have to enroll fewer patients in total (per physician) to reflect the larger amount of time per patient that the physician and other practice staff will need to devote to their care.82 Under Patient-Centered Payment, the smaller number of patients will not reduce the practice’s revenue because the practice will receive bigger payments for the higher-need patients.
Figure 21 shows two different hypothetical specialty practices providing services for patients with chronic conditions. The second practice has a larger proportion of patients who have complex conditions or are receiving complex treatments; that practice also has fewer patients in total because of the greater amount of time it would have to spend with the higher-need patients. Under the Patient-Centered Payment structure, since the payments would be higher for the higher-need patients, the second practice would not lose money by serving fewer patients.
This approach helps physicians, nurses, and other practice staff avoid the “burnout” caused when the time required to do everything patients need exceeds the length of a normal workday. As shown at the bottom of Figure 21, the physician and nurse in each practice would be able to spend the amount of time needed with all patients in an average of 8-9 hours per day.
FIGURE 21
Revenues and Expenses at Hypothetical Physician Practices
with Lower-Complexity and Higher-Complexity Patients
| Specialist Practice A | Specialist Practice B | ||||||
|---|---|---|---|---|---|---|---|
| Lower-Complexity Patients | Higher-Complexity Patients | ||||||
| Practice Revenue | Payment Amount | Patients | Months Per Patient |
Total | Patients | Months Per Patient |
Total |
| Diagnosis Payments | |||||||
| Assistance to PCP | $37 | 178 | $6,586 | 146 | $5,402 | ||
| Low Complexity Dx | $146 | 267 | $38,982 | 73 | $10,658 | ||
| Moderate Complexity Dx | $218 | 356 | $77,608 | 219 | $47,742 | ||
| High Complexity Dx | $291 | 89 | $25,899 | 292 | $84,972 | ||
| Care Planning Payments | |||||||
| Assistance to PCP | $37 | 80 | $2,964 | 66 | $2,431 | ||
| Low Complexity Plan | $75 | 160 | $12,015 | 66 | $4,928 | ||
| Moderate Complexity Plan | $145 | 481 | $69,687 | 263 | $38,106 | ||
| High Complexity Plan | $214 | 80 | $17,141 | 263 | $56,239 | ||
| Initial Management | |||||||
| Non-Complex | $206 | 392 | 1.0 | $80,663 | 230 | 1.0 | $47,259 |
| Complex Tx | $290 | 168 | 1.0 | $48,804 | 230 | 1.0 | $66,717 |
| Ongoing Management | |||||||
| Non-Complex | $40 | 269 | 11.4 | $122,726 | 138 | 11.4 | $62,914 |
| Complex Patient | $94 | 34 | 10.8 | $34,153 | 83 | 10.8 | $84,040 |
| Complex Treatment | $94 | 17 | 10.8 | $17,077 | 28 | 10.8 | $28,013 |
| Complex Pt and Tx | $133 | 17 | 10.2 | $22,819 | 28 | 10.2 | $37,434 |
| Total Revenue | $577,125 | $576,856 | |||||
| Practice Expenses | Unit Cost | FTE | Total | FTE | Total | ||
| Physician | $250,000 | 1.0 | $250,000 | 1.0 | $250,000 | ||
| Nurse | $80,000 | 1.0 | $80,000 | 1.0 | $80,000 | ||
| Medical Assistant | $38,000 | 1.0 | $38,000 | 1.0 | $38,000 | ||
| Receptionist | $36,000 | 1.0 | $36,000 | 1.0 | $36,000 | ||
| Billing | $36,000 | 0.5 | $18,000 | 0.5 | $18,000 | ||
| Benefits | $64,400 | $64,400 | |||||
| Rent/Utilities | $45,000 | $45,000 | |||||
| EHR and IT | $14,000 | $14,000 | |||||
| Liability Insurance | $9,000 | $9,000 | |||||
| Supplies/Other | $12,000 | $12,000 | |||||
| Total Expenses | $566,400 | $566,400 | |||||
| Profit/Loss | $10,725 | $10,456 | |||||
| +2% | +2% | ||||||
| Provider Workload | |||||||
| Physician Hours Per Day | 8.7 | 8.6 | |||||
| Nurse Hours Per Day | 8.0 | 8.4 | |||||
Practices Focusing on Specific Services
In addition to differences in the complexity and needs of the patients, some specialty practices may focus on delivering specific subsets of services. For example, in a community where patients have access to high-quality primary care practices that are paid adequately and appropriately to manage the care of patients with chronic conditions, specialists can choose to focus primarily on diagnosis, treatment planning, and initial treatment of patients, with the ongoing management of chronic conditions for most patients handled by the patients’ primary care practices.
Figure 22 shows two hypothetical specialty practices. The first practice primarily manages ongoing care for a group of patients, whereas the second practice focuses primarily on diagnosis, care planning, and initial treatment of patients (with ongoing care managed by a primary care practice). The second practice sees many more different patients during the course of a year, but it sees each of them for at most a few months. The first practice sees a smaller number of individual patients, but most of those patients receive services from the practice on a year-round basis. Under the Patient-Centered Payment system, both practices would receive adequate revenues to cover their costs with manageable workloads for the physician and practice staff.
FIGURE 22
Revenues and Expenses at Hypothetical Physician Practices
Providing Different Subsets of Chronic Condition Care
| Specialist Practice C | Specialist Practice D | ||||||
|---|---|---|---|---|---|---|---|
| Mostly Ongoing Condition Management | Mostly Diagnosis and Initial Care | ||||||
| Practice Revenue | Payment Amount | Patients | Months Per Patient |
Total | Patients | Months Per Patient |
Total |
| Diagnosis Payments | |||||||
| Assistance to PCP | $37 | 115 | $4,255 | 300 | $11,100 | ||
| Low Complexity Dx | $146 | 173 | $25,185 | 450 | $65,700 | ||
| Moderate Complexity Dx | $218 | 230 | $50,140 | 600 | $130,800 | ||
| High Complexity Dx | $291 | 57 | $16,733 | 150 | $43,650 | ||
| Care Planning Payments | |||||||
| Assistance to PCP | $37 | 52 | $1,915 | 135 | $4,995 | ||
| Low Complexity Plan | $75 | 104 | $7,763 | 270 | $20,250 | ||
| Moderate Complexity Plan | $145 | 311 | $45,023 | 810 | $117,450 | ||
| High Complexity Plan | $214 | 52 | $11,075 | 135 | $28,890 | ||
| Initial Management | |||||||
| Non-Complex | $206 | 290 | 1.0 | $59,559 | 189 | 1.0 | $38,843 |
| Complex Tx | $290 | 124 | 1.0 | $36,035 | 81 | 1.0 | $23,501 |
| Ongoing Management | |||||||
| Non-Complex | $40 | 530 | 11.4 | $241,644 | 43 | 11.4 | $19,699 |
| Complex Patient | $94 | 66 | 10.8 | $67,247 | 5 | 10.8 | $5,482 |
| Complex Treatment | $94 | 33 | 10.8 | $33,623 | 3 | 10.8 | $2,741 |
| Complex Pt and Tx | $133 | 33 | 10.2 | $44,931 | 3 | 10.2 | $3,663 |
| Total Revenue | $645,125 | $516,764 | |||||
| Practice Expenses | Unit Cost | FTE | Total | FTE | Total | ||
| Physician | $250,000 | 1.0 | $250,000 | 1.0 | $250,000 | ||
| Nurse | $80,000 | 1.5 | $120,000 | 0.5 | $40,000 | ||
| Medical Assistant | $38,000 | 1.0 | $38,000 | 1.0 | $38,000 | ||
| Receptionist | $36,000 | 1.0 | $36,000 | 1.0 | $36,000 | ||
| Billing | $36,000 | 0.5 | $18,000 | 0.5 | $18,000 | ||
| Benefits | $72,400 | $56,400 | |||||
| Rent/Utilities | $47,500 | $42,500 | |||||
| EHR and IT | $16,000 | $12,000 | |||||
| Liability Insurance | $10,500 | $7,500 | |||||
| Supplies/Other | $13,000 | $11,000 | |||||
| Total Expenses | $621,400 | $511,400 | |||||
| Profit/Loss | $23,725 | $5,364 | |||||
| +4% | +1% | ||||||
| Provider Workload | |||||||
| Physician Hours Per Day | 9.2 | 8.5 | |||||
| Nurse Hours Per Day | 6.9 | 9.1 | |||||
Practices With Different Numbers and Types of Staff
In rural areas, the number of patients who have a particular chronic condition, even a common chronic condition, may be not be large enough to support the work of more than a single specialist. If payments are not designed in a way that will sustain a solo specialist practice, the patients in these communities will be unable to receive appropriate specialty care without traveling long distances. Even in larger communities where there are enough patients to support a larger practice, the payment system should allow physicians to form smaller practices if they wish to do so, rather than forcing them to consolidate because the payments are not adequate.
The examples in Figures 21 and 22 show that the Patient-Centered Payment amounts that were defined in earlier sections would be adequate to support a very small practice – one physician, a nurse, and a medical assistant (MA) – as well as larger practices.
The calculations of payment amounts were based on using a Registered Nurse (RN) to provide most of the care planning and care management services that the physician does not provide. Although various aspects of care planning and care management for patients could be performed by social workers, pharmacists, and nutritionists as well as a nurse, none of those individuals could carry out all of the tasks required for all patients. Consequently, if a small practice only has enough patients to support one clinical staff member (in addition to the physician and MA), that individual would likely need to be an RN.
However, if a larger practice has enough patients to require hiring multiple nurses, it would have the flexibility under Patient-Centered Payment to hire different types of staff if it wished to do so. Figure 23 shows how a practice with 11,000 - 12,000 patients would need about 6 RNs if it only used RNs, but it could also hire a combination of RNs, social workers, nutritionists, and pharmacists instead, as long as there were enough patients whose needs could be met by individuals with those skills instead of RNs. In addition, the second practice has a large enough number of patients to enable it to hire a combination of physicians and nurse practitioners and/or physician assistants, not just physicians.
FIGURE 23
Revenues and Expenses at Hypothetical Physician Practices
with Different Types of Staff Teams
| Specialist Practice E | Specialist Practice F | ||||||
|---|---|---|---|---|---|---|---|
| All Physicians and RNs | Multiple Types of Staff on Team | ||||||
| Practice Revenue | Payment Amount | Patients | Months Per Patient | Total | Patients | Months Per Patient | Total |
| Diagnosis Payments | |||||||
| Assistance to PCP | $37 | 2,320 | $85,840 | 2,320 | $85,840 | ||
| Low Complexity Dx | $146 | 3,480 | $508,080 | 3,480 | $508,080 | ||
| Moderate Complexity Dx | $218 | 4,640 | $1,011,520 | 4,640 | $1,011,520 | ||
| High Complexity Dx | $291 | 1,160 | $337,560 | 1,160 | $337,560 | ||
| Care Planning Payments | |||||||
| Assistance to PCP | $37 | 580 | $21,460 | 580 | $21,460 | ||
| Low Complexity Plan | $75 | 1,160 | $87,000 | 1,160 | $87,000 | ||
| Moderate Complexity Plan | $145 | 3,480 | $504,600 | 3,480 | $504,600 | ||
| High Complexity Plan | $214 | 580 | $124,120 | 580 | $124,120 | ||
| Initial Management | |||||||
| Non-Complex | $206 | 2,030 | 1.0 | $417,199 | 2,030 | 1.0 | $417,199 |
| Complex Tx | $290 | 870 | 1.0 | $252,421 | 870 | 1.0 | $252,421 |
| Ongoing Management | |||||||
| Non-Complex | $40 | 1,392 | 11.4 | $634,752 | 1,392 | 11.4 | $634,752 |
| Complex Patient | $94 | 174 | 10.8 | $176,645 | 174 | 10.8 | $176,645 |
| Complex Treatment | $94 | 87 | 10.8 | $88,322 | 87 | 10.8 | $88,322 |
| Complex Pt and Tx | $133 | 87 | 10.2 | $118,024 | 87 | 10.2 | $118,024 |
| Total Revenue | $4,367,543 | $4,367,543 | |||||
| Practice Expenses | Unit Cost | FTE | Total | FTE | Total | ||
| Physician | $250,000 | 8.0 | $2,000,000 | 7.0 | $1,750,000 | ||
| Nurse Practitioner | $120,000 | 0.0 | $0 | 1.0 | $120,000 | ||
| RN | $80,000 | 6.0 | $480,000 | 4.0 | $320,000 | ||
| Social Worker | $70,000 | 0.0 | $0 | 1.0 | $70,000 | ||
| Nutritionist | $70,000 | 0.0 | $0 | 1.0 | $70,000 | ||
| Pharmacist | $160,000 | 0.0 | $0 | 1.0 | $160,000 | ||
| Medical Assistant | $38,000 | 8.0 | $304,000 | 5.0 | $190,000 | ||
| Community Health Worker | $38,000 | 0.0 | $0 | 2.0 | $76,000 | ||
| Receptionist | $36,000 | 4.0 | $144,000 | 4.0 | $144,000 | ||
| Billing | $36,000 | 4.0 | $144,000 | 4.0 | $144,000 | ||
| Benefits | $454,400 | $468,800 | |||||
| Rent/Utilities | $350,000 | $350,000 | |||||
| EHR and IT | $104,000 | $104,000 | |||||
| Liability Insurance | $66,000 | $66,000 | |||||
| Supplies/Other | $92,000 | $92,000 | |||||
| Total Expenses | $4,138,400 | $4,124,800 | |||||
| Profit/Loss | $229,143 | $242,743 | |||||
| +6% | +6% | ||||||
Summary of Patient-Centered Payment for Chronic Condition Care
Figure 24 summarizes all of the elements of Patient-Centered Payment for Care of Chronic Conditions.
Although there are multiple separate payments targeted at different subsets of services and different types of patients, all of the payments are necessary to give a physician practice adequate flexibility and resources to deliver high-quality care to each individual patient. If only a subset of the payments is implemented, the quality of care for all patients would be reduced, because the physician practice would not be able to employ the appropriate staff and it could be forced to deliver fewer services or less effective services than necessary for more patients than it can effectively manage.
FIGURE 24
Patient-Centered Payment for Care of Chronic Conditions
| Type of Service | Code | Payment/Service | Frequency of Payment | Accountability for Quality | Estimated Amount of Payment |
|---|---|---|---|---|---|
| Diagnosis | XX040 | Diagnosis Assistance | Once per patient | Follow evidence-based guidelines for diagnosis and testing | $37 |
| XX041 | Low Complexity Diagnosis | $146 | |||
| XX042 | Moderate Complexity Diagnosis | $218 | |||
| XX043 | High Complexity Diagnosis | $291 | |||
| Care Planning | XX050 | Care Planning Assistance | Once per patient | Use evidence-based guidelines for treatment and management of the chronic condition | $37 |
| XX051 | Low Complexity Care Planning | $75 | |||
| XX052 | Moderate Complexity Care Planning | $145 | |||
| XX053 | High Complexity Care Planning | $214 | |||
| XX054 | Additional Care Planning Time | Each extra 30 minutes of clinical staff time | $31 | ||
| Chronic Condition Treatment and Management | XX030 | Initial Condition Management | Monthly for 1-3 Months | Follow evidence-based guidelines for treatment and management of the chronic condition | $206 |
| XX031 | Condition Management (Non-Complex Condition and Treatment) |
Monthly (except months in which patient is hospitalized) | $40 | ||
| XX032 | Condition Management for Complex Chronic Condition |
$94 | |||
| Chronic Condition Treatment and Management (Complex Treatment) | XX034 | Initial Condition Management (with Complex Treatment) |
Monthly for 1-3 Months | Follow evidence-based guidelines for treatment and management of the condition(s) and monitor patient needs | $290 |
| XX035 | Condition Management (with Complex Treatment) |
Monthly (except months in which patient is hospitalized) | $94 | ||
| XX036 | Condition Management for Complex Chronic Condition (with Complex Treatment) |
$133 | |||
| Injected or Infused Medication | JXXX0 | Practice-Administered Drug Cost Payment - Payment for Drug Acquisition Cost |
When drug is administered | Follow evidence-based guidelines for choosing medications | Payment based on acquisition cost of drug |
| JXXX1 | Practice-Administered Drug Cost Payment - Payment for Wastage/Breakage Losses |
~1% of drug acquisition cost | |||
| XX060 | Practice-Administered Drug Cost Payment – Payment for Pharmacy Operations Costs |
Monthly | Meet standards for operation of specialty pharmacy | Based on pharmacy operation cost and expected total number of patients | |
| Test or Other Procedure | Varies | Standard CPT code for procedure or test | When procedure or test is performed | Follow evidence-based guidelines in ordering test or performing procedure | Payment based on cost of procedure or test |
As shown in Figure 25, the payments received by a specialty practice would depend on the specific phases of care that would be managed by the patient’s primary care practice vs. the specialist practice. For example:
- a primary care physician who identified new symptoms that could potentially indicate the presence of a chronic disease might refer the patient to the specialist for diagnosis (or receive assistance from the specialist in making the diagnosis), and if the specialist determines that the patient does have the chronic disease, the primary care practice would develop the care plan and provide the services needed to manage the condition. In this case, the specialist practice would bill for and be paid a Diagnosis Payment (or Diagnosis Assistance Payment), but not a Care Planning Payment or Condition Management Payments.
- a primary care practice that is managing a patient’s chronic condition might temporarily transfer care to a specialist practice (e.g., if the patient develops an acute condition that makes management of the chronic condition more complex, or if the patient is living in a different community temporarily) and then the primary care practice would resume responsibility later. In this case, the specialist practice would bill for and be paid Condition Management Payments during the time the patient is receiving services from that practice.
FIGURE 25
Payments in Each Phase of Care
Under Patient-Centered Payment for Care of Chronic Conditions
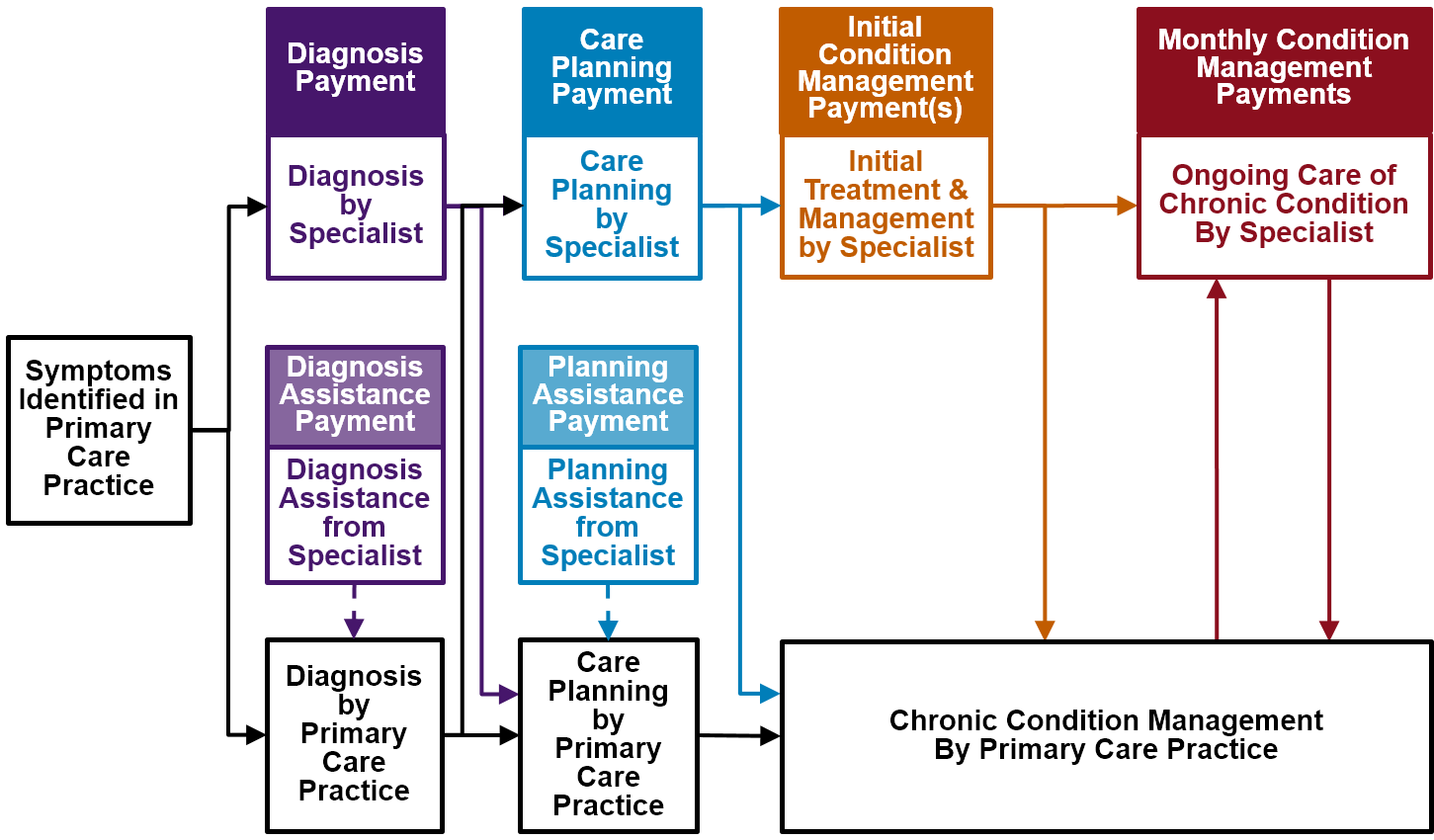
In each phase of care, the Patient-Centered Payment would be higher for a patient with greater needs, as shown in Figure 26. The higher payments would support the additional time that the physician practice would need to spend with higher-need patients. In addition, the Diagnosis Payments and Initial Condition Management Payments would be much higher than the monthly Condition Management Payments, reflecting the importance of these two initial phases of care in determining future outcomes and the significant amount of time needed to complete these phases with an accurate diagnosis and an effective care plan.
FIGURE 26
Relative Magnitude of Individual Payments
in Patient-Centered Payment for Care of Chronic Conditions
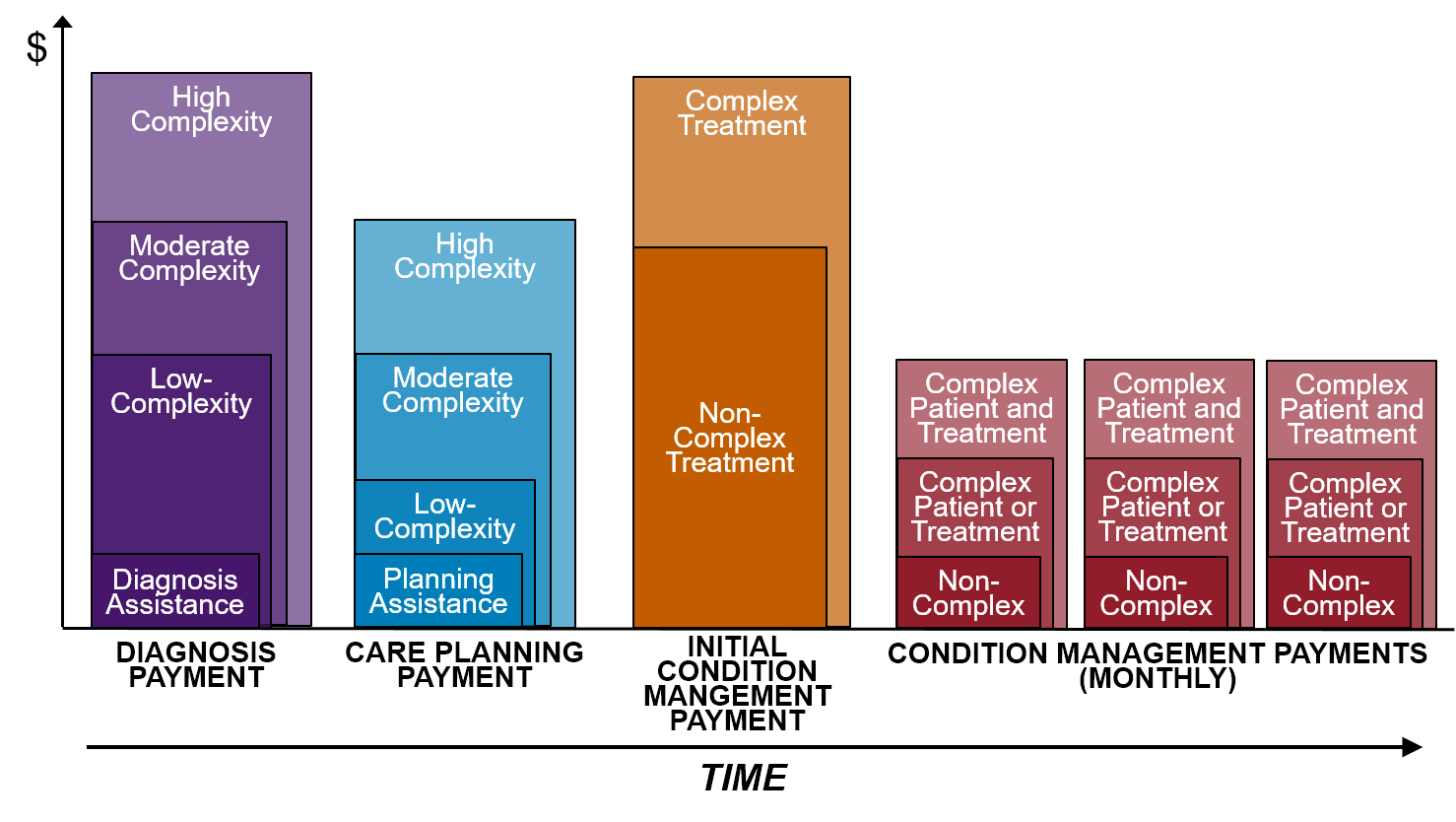
The Costs and Benefits of Patient-Centered Payment
Impacts on Payer Spending for Physician Practice Services
The patient-centered payments described in Section 3 are designed to provide adequate payments to physician practices that deliver high-quality diagnosis, treatment planning, and condition management services to patients who have a chronic condition. Although this approach would do a better job of supporting these services than current fee-for-service payments or value-based payments, it is not obvious from the analyses in Section 3 whether payers or patients would have to spend more on specialist physician services for patients with chronic conditions under the Patient-Centered Payment system than they do today.
In general, under Patient-Centered Payment for Care of Chronic Conditions, spending on services delivered by physician practices for care of chronic conditions would be higher than it is today for some patients and lower for others, for several reasons:
- Medicare and other payers currently pay fees for some of the physician services that would be supported by the patient-centered payment system for some patients, but not for all of the services or for all patients who need them. As a result, in some cases, spending under Patient-Centered Payment for a particular patient would be higher than what a physician practice would be paid under current payment systems, but in other cases it would be similar or lower.
- Most current fees are tied specifically to office visits with patients, and the care management fees paid by Medicare and some payers are tied to minimum amounts of time spent on care management services for a patient during a month. Because of this, a physician practice that delivers services in a way designed to maximize current fee-for-service payments could be paid more for some patients under the current fee structure than it would be paid under the patient-centered payment system.
- The fees paid by Medicare and most other payers are not specifically designed to support the greater amount of time needed by patients who have complex conditions or barriers to accessing healthcare services. Because the patient-centered payment amounts would be higher for patients with higher needs, spending on physician practice services is likely to be higher on many of those patients than under current payment systems.
- Since many Medicaid programs pay fees to physician practices that are much lower than Medicare rates, it is likely that paying the patient-centered payment amounts for chronic condition care would increase Medicaid spending on these physician practice services. Conversely, some private insurance plans pay specialty physician practices much higher fees than Medicare does, and for them, the patient-centered payment amounts could represent a reduction in spending.
More specific comparisons for the Medicare program are provided below.
Diagnosis Payments
Figure 27 compares the Diagnosis Payments under Patient-Centered Payment to current Medicare payments for office visits with new patients, under two different scenarios: (1) the physician’s diagnosis work is completed with a single patient visit with medical decision-making complexity similar to the Diagnosis Payment, and (2) a follow-up visit with the patient is also required (with equal or lower complexity). The Diagnosis Payments would likely be about 28-30% higher than Medicare payments if only one visit is made, but 17-29% lower if two visits are required. Since a subset of patients will likely require a follow-up visit with the specialist to complete the diagnosis process, this suggests that on average, spending will be similar. With the Patient-Centered Diagnosis Payments, however, there will be no financial incentive for a practice to bring a patient back for a second visit if it is not necessary.
As shown in Figure 27, the Diagnosis Assistance Payment would be about the same as what Medicare pays for an 11-20 minute interprofessional consultation. Medicare only pays half as much if the consultation lasts 10 minutes or less, which provides a perverse incentive for a physician to spend unnecessary time on the consultation. In contrast, the Diagnosis Assistance Payment would not require that any specific minimum amount of time be spent.
FIGURE 27
Spending on Diagnosis of Chronic Conditions
Under Current Payment Systems and Patient-Centered Payment
| Medicare Spending | Patient-Centered Payment |
Difference | ||||||
| CPT | Medicare Fee Schedule | 2022 Fee | Visits | Total Per Patient | Total Per Patient | $ | % | |
| XX041 Low Complexity Diagnosis | ||||||||
| 1 | 99203 | Level 3 E/M Visit - New Patient | $113.85 | 1 | $113.85 | $146.00 | $32 | +28% |
| 2 | 99203 | Level 3 E/M Visit - New Patient | $113.85 | 1 | $113.85 | |||
| 99213 | Level 3 E/M Visit - Established Patient | $92.05 | 1 | $92.05 | ||||
| Total: | $205.91 | $146.00 | ($60) | -29% | ||||
| XX042 Moderate Complexity Diagnosis | ||||||||
| 1 | 99204 | Level 4 E/M Visit - New Patient | $169.57 | 1 | $169.57 | $218.00 | $48 | +29% |
| 2 | 99204 | Level 4 E/M Visit - New Patient | $169.57 | 1 | $169.57 | |||
| 99213 | Level 3 E/M Visit - Established Patient | $92.05 | 1 | $92.05 | ||||
| Total: | $261.62 | $218.00 | ($44) | -17% | ||||
| XX043 High Complexity Diagnosis | ||||||||
| 1 | 99205 | Level 5 E/M Visit - New Patient | $224.25 | 1 | $224.25 | $291.00 | $67 | +30% |
| 2 | 99205 | Level 5 E/M Visit - New Patient | $224.25 | 1 | $224.25 | |||
| 99214 | Level 4 E/M Visit - Established Patient | $129.77 | 1 | $129.77 | ||||
| Total: | $354.02 | $291.00 | ($63) | -18% | ||||
| XX040 Diagnosis Assistance | ||||||||
| 1 | 99447 | Interprofessional Assessment (11-20 minutes) | $36.68 | 1 | $36.68 | $37.00 | $0 | +1% |
| 2 | 99446 | Interprofessional Assessment (5-10 minutes) | $18.69 | 1 | $18.69 | $37.00 | $18 | +98% |
Care Planning Payments
Figure 28 compares the Care Planning Payments under Patient-Centered Payment to current Medicare payments for office visits with established patients, under scenarios similar to those used above for Diagnosis Payments, i.e., (1) the care planning work is completed with a single patient visit with decision-making complexity similar to the Care Planning Payment, or (2) a follow-up visit with the patient is also required to complete the plan for a patient with a more complex condition. As Figure 28 shows, the Low Complexity Care Planning Payment would be 19% lower than the current Medicare payment (since most of the care planning work for these patients could likely be done by a nurse). The Moderate Complexity Care Planning Payment and the High Complexity Care Planning Payment would be 12-17% higher than Medicare payments if only one visit is made, but 22-35% lower if two visits are required. Since a subset of patients will likely require a follow-up visit, this suggests that on average, those Care Planning Payments will be similar to current Medicare payments. As with the Diagnosis Payments, the Care Planning Payments will not create a financial incentive for a practice to bring a patient back for a second visit if it is not necessary.
FIGURE 28
Spending on Care Planning for Chronic Conditions
Under Current Payment Systems and Patient-Centered Payment
| Medicare Spending | Patient-Centered Payment |
Difference | ||||||
| CPT | Medicare Fee Schedule | 2022 Fee | Visits | Total Per Patient | Total Per Patient | $ | % | |
| XX051 Low Complexity Care Planning | ||||||||
| 99213 | Level 3 E/M Visit - Established Patient | $92.05 | 1 | $92.05 | $75.00 | ($17) | -19% | |
| XX052 Moderate Complexity Care Planning | ||||||||
| 1 | 99214 | Level 4 E/M Visit - Established Patient | $129.77 | 1 | $129.77 | $145.00 | $15 | +12% |
| 2 | 99214 | Level 4 E/M Visit - Established Patient | $129.77 | 1 | $129.77 | |||
| 99213 | Level 3 E/M Visit - Established Patient | $92.05 | 1 | $92.05 | ||||
| Total: | $221.83 | $145.00 | ($77) | -35% | ||||
| XX053 High Complexity Care Planning | ||||||||
| 1 | 99215 | Level 5 E/M Visit - Established Patient | $183.07 | 1 | $183.07 | $214.00 | $31 | +17% |
| 2 | 99215 | Level 5 E/M Visit - Established Patient | $183.07 | 1 | $183.07 | |||
| 99213 | Level 3 E/M Visit - Established Patient | $92.05 | 1 | $92.05 | ||||
| Total: | $275.12 | $214.00 | ($61) | -22% | ||||
| XX050 Care Planning Assistance | ||||||||
| 1 | 99447 | Interprofessional Assessment (11-20 minutes) | $36.68 | 1 | $36.68 | $37.00 | $0 | +1% |
| 2 | 99446 | Interprofessional Assessment (5-10 minutes) | $18.69 | 1 | $18.69 | $37.00 | $18 | +98% |
The comparisons in Figure 28 are based on the current fees for “established” patients, i.e., a patient who has made a visit to the practice at least once before. If a primary care physician has already diagnosed the patient and refers the patient to the specialist practice for development of a care plan, then the patient would be treated as a “new patient” for the specialist practice under the current fee-for-service system, and the practice would be paid higher amounts for these visits, similar to what is shown in Figure 27. However, there would be no difference in the Patient-Centered Payment amount, since it is designed to support the time involved in care planning regardless of whether the practice also made the diagnosis of the condition. In these cases, the Patient-Centered Payment amounts would be virtually identical to current fees.
As shown in Figure 28, the Care Planning Assistance Payment would be about the same as what Medicare pays for an 11-20 minute interprofessional consultation. Medicare only pays half as much if the consultation lasts 10 minutes or less, which provides a perverse incentive for a physician to spend unnecessary time on the consultation. In contrast, the Care Planning Assistance Payment would not require that any specific minimum amount of time be spent.
Condition Management Payments
Comparing spending for the Condition Management Payments under Patient-Centered Payment to spending in the current fee-for-service payment system is much more complicated, because there are currently multiple fees that a practice could potentially receive during a month depending on exactly how it delivers services to the patient. Under the Medicare payment system:
- If the patient sees the physician during the month, the practice can receive an evaluation and management services (E/M) payment for the visit. Under the temporary regulations established during the COVID-19 Public Health Emergency, the same amount would be paid for an office visit, a video visit in the patient’s home, or a telephone call, but if these regulations expire, the fees would only be paid for an office visit.
- If the patient sees a nurse instead of the physician, the practice would not be eligible for a visit payment.
- If the patient sees the physician more than once during the month, the practice would receive an additional payment for each visit.
- If the practice provides at least 30 minutes of care management services to the patient during the month, if the patient has agreed to pay cost-sharing for those services during that month, and if the patient’s chronic condition meets specific eligibility criteria, the practice can receive a “Principal Care Management” payment. If less than 30 minutes of services are provided during the month, there is no payment, even if the amount of time over several months averages 30 minutes or more per month.
- If the practice provides 60 minutes of care management services during the month, it can receive an additional Principal Care Management (PCM) payment. However, if it only provides 31-59 minutes of services, it will only receive the single PCM payment, even if the amount of time over several months averages 60 minutes or more per month.
- If the practice provides 20 minutes of care management services to the patient during the month, and if (a) the patient has two or more chronic conditions, (b) the patient has agreed to pay cost-sharing for the services during the month, and (c) no other physician is providing similar services to the patient, the practice can receive a “Non-Complex Chronic Care Management” payment. If the practice provides 40 minutes of services, it can receive an additional payment, but there is no additional payment if only 21-39 minutes of services are delivered.
Figure 29 shows that the Initial Condition Management Payment amounts under Patient-Centered Payment would be similar to fee-for-service spending for non-complex patients if the patient was eligible and agreed to receive the care management services and pay the cost-sharing amounts required by Medicare; the payment would be higher for patients who would not have agreed to pay cost-sharing for care management. Spending would be similar for the complex patients if one assumes those patients would either agree to receive care management services or make an additional visit to the practice during the initial month of treatment.
FIGURE 29
Spending on Initial Condition Management for Chronic Conditions Under Current Payment Systems and Patient-Centered Payment
| Medicare Spending | Patient-Centered Payment | Difference | |||||||||
| CPT | Medicare Fee Schedule | 2022 Fee | Visits | % Patients Enrolled |
Months with Minimum Time |
Total Per Patient | Months | Total Per Patient | $ | % | |
| XX030 Initial Condition Management - Non-Complex Treatment | |||||||||||
| 1 | 99214 | Level 4 E/M Visit - Established Patient | $129.77 | 1 | $129.77 | 1 | $205.52 | $76 | +58% | ||
| 2 | 99214 | Level 4 E/M Visit - Established Patient | $129.77 | 1 | $129.77 | ||||||
| 99426 | Principal Care Mgt (30 minutes per month) | $63.33 | 100% | 1 | $63.33 | ||||||
| Total: | $193.10 | 1 | $205.52 | $13 | +6% | ||||||
| XX034 Initial Condition Management - Complex Treatment | |||||||||||
| 1 | 99215 | Level 5 E/M Visit - Established Patient | $183.07 | 1 | $183.07 | ||||||
| 99213 | Level 3 E/M Visit - Established Patient | $92.05 | 1 | $92.05 | |||||||
| Total: | $275.12 | 1 | $290.14 | $15 | 5% | ||||||
| 2 | 99215 | Level 5 E/M Visit - Established Patient | $183.07 | 1 | $183.07 | ||||||
| 99426 | Principal Care Mgt (30 minutes per month) | $63.33 | 100% | 1 | $63.33 | ||||||
| 99427 | Principal Care Mgt (extra 30 minutes) | $48.45 | 100% | 1 | $48.45 | ||||||
| Total: | $294.84 | 1 | $290.14 | ($5) | -2% | ||||||
Figure 30 shows that the Condition Management Payment amounts after the initial treatment period would be similar to what a practice could potentially receive under fee-for-service payments if the practice has frequent visits with the patients, if most of the patients agree to receive care management services from the practice, and if the practice spends 30 minutes providing care management services to the patients in most months. Conversely, spending under Patient-Centered Payment would be significantly higher than fee-for-service spending for a patient who does not make many visits to the practice or does not agree to pay cost-sharing for care management services.
FIGURE 30
Spending on Ongoing Condition Management for Chronic Conditions Under Current Payment Systems and Patient-Centered Payment
| Medicare Spending | Patient-Centered Payment | Difference | |||||||||
| CPT | Medicare Fee Schedule | 2022 Fee | Visits | % Patients Enrolled |
Months with Minimum Time |
Total Per Patient | Months | Total Per Patient | $ | % | |
| XX031 Condition Management - Non-Complex | |||||||||||
| 1 | 99213 | Level 3 E/M Visit - Established Patient | $92.05 | 3 | $276.16 | 12 | $480.00 | $204 | 74% | ||
| 2 | 99213 | Level 3 E/M Visit - Established Patient | $92.05 | 2 | $184.10 | ||||||
| 99426 | Principal Care Mgt (30 minutes per month) | $63.33 | 70% | 8 | $354.64 | ||||||
| Total: | $538.75 | 12 | $480.00 | ($59) | -11% | ||||||
| XX032 Condition Management - Complex Patient | |||||||||||
| 1 | 99214 | Level 4 E/M Visit - Established Patient | $129.77 | 6 | $778.64 | 12 | $1,128.00 | $349 | 45% | ||
| 2 | 99214 | Level 4 E/M Visit - Established Patient | $129.77 | 4 | $519.09 | ||||||
| 99426 | Principal Care Mgt (30 minutes per month) | $63.33 | 80% | 10 | $506.63 | ||||||
| 99427 | Principal Care Mgt (extra 30 minutes) | $48.45 | 80% | 3 | $116.28 | ||||||
| Total: | $1,142.00 | 12 | $1,128.00 | ($14) | -1% | ||||||
| XX035 Condition Management - Complex Treatment | |||||||||||
| 1 | 99215 | Level 5 E/M Visit - Established Patient | $183.07 | 4 | $732.27 | 12 | $1,128.00 | $396 | 54% | ||
| 2 | 99215 | Level 5 E/M Visit - Established Patient | $183.07 | 1 | $183.07 | ||||||
| 99214 | Level 4 E/M Visit - Established Patient | $129.77 | 2 | $259.55 | |||||||
| 99426 | Principal Care Mgt (30 minutes per month) | $63.33 | 80% | 10 | $506.63 | ||||||
| 99427 | Principal Care Mgt (extra 30 minutes) | $48.45 | 80% | 5 | $193.79 | ||||||
| Total: | $1,143.04 | 12 | $1,128.00 | ($15) | -1% | ||||||
| XX036 Condition Management - Complex Patient and Complex Treatment | |||||||||||
| 1 | 99215 | Level 5 E/M Visit - Established Patient | $183.07 | 6 | $1,098.40 | 12 | $1,596.00 | $498 | 45% | ||
| 2 | 99215 | Level 5 E/M Visit - Established Patient | $183.07 | 3 | $549.20 | ||||||
| 99214 | Level 4 E/M Visit - Established Patient | $129.77 | 2 | $259.55 | |||||||
| 99426 | Principal Care Mgt (30 minutes per month) | $63.33 | 80% | 12 | $607.96 | ||||||
| 99427 | Principal Care Mgt (extra 30 minutes) | $48.45 | 80% | 6 | $232.55 | ||||||
| Total: | $1,649.26 | 12 | $1,596.00 | ($53) | -3% | ||||||
Although it is reasonable to expect that complex patients would need to be seen more often and receive more extensive care management services than non-complex patients, the patients may not be able or willing to have frequent visits with the physician or to pay for monthly care management services. Consequently, under fee-for-service payment, the practice would be forced to either lose money or provide less support than many complex patients would need. In contrast, under Patient-Centered Payment, the practice would be paid to provide evidence-based care to the patient, even if it did so in ways that would not qualify for fee-for-service payments.
Figure 30 also shows that the Condition Management Payments provide a far more predictable revenue stream for the practice and more predictable spending for the payer than fee-for-service payments. Under the current payment system, the practice’s revenue for a patient with a chronic condition could vary significantly from month to month based on whether the patient had a visit with the practice, whether the patient agreed to pay for care management services, and whether the practice spent 30 minutes or more to deliver care management services to the patient. The practice’s payment during a month would depend on how much time was spent, not on the quality of care provided. In contrast, under the Patient-Centered Payment system, the practice would be paid the same amount for a patient every month as long as the practice delivered all of the services to that patient that are specified under an evidence-based Clinical Practice Guideline or Pathway, regardless of the exact amount of time that was required.
Overall Payments
The combined impact of all of these differences can be assessed by comparing how much a specialist physician practice would receive in total for all of the different types of patients with chronic conditions who are receiving services from the practice under Patient-Centered Payment for Care of Chronic Conditions and under current fee-for-service payments.
Figure 31 shows the amounts of revenue that would be received under both Patient-Centered Payment and standard Medicare payments for some of the hypothetical practices that were used as examples in Section 3.H. The fee-for-service revenue calculations are based on assumptions that some but not all patients would enroll to receive the monthly Principal Care Management (PCM) service paid for by Medicare and that not all of the patients who were enrolled would need or receive the 30 minutes of services every month that are required to receive the PCM payment.
In general, physician practices could expect to receive higher revenues under Patient-Centered Payment and thereby avoid the losses that could occur under fee-for-service payments. This means that the payer (Medicare or a health plan paying Medicare rates) would likely spend more overall under Patient-Centered Payment on physician practice services for care of chronic conditions, but with a higher standard of quality than under the current payment system.
FIGURE 31
Revenues and Expenses at Hypothetical Specialty Practices Under Current Payment Systems and Patient-Centered Payment
| Specialist Practice A | Specialist Practice B | Specialist Practice C | Specialist Practice D | |
| Lower-Complexity Patients | Higher-Complexity Patients | Mostly Ongoing Condition Mgt | Mostly Diagnosis and Initial Care | |
| Expenses | Expenses | Expenses | Expenses | |
| Total Practice Expenses | $566,400 | $566,400 | $621,400 | $511,400 |
| Fee-for-Service Payment | Revenue | Revenue | Revenue | Revenue |
| Total Visit Fees | $392,601 | $411,367 | $395,599 | $410,374 |
| Total Care Mgt Payments | $136,086 | $147,534 | $238,748 | $32,056 |
| Total FFS Revenue | $528,687 | $558,901 | $634,347 | $442,431 |
| Profit/Loss | ($37,713) | ($7,499) | $12,947 | ($68,969) |
| -7% | -1% | +2% | -13% | |
| Patient-Centered Payment | Revenue | Revenue | Revenue | Revenue |
| Total Revenue | $577,125 | $576,856 | $673,174 | $516,764 |
| Profit/Loss | $10,725 | $10,456 | $51,774 | $5,364 |
| +2% | +2% | +8% | +1% | |
| Difference in Revenue | +9% | +3% | +6% | +17% |
Impacts on Total Healthcare Spending
The previous section focused narrowly on how much more or less a payer would spend on the services delivered by the physician practice to patients with a chronic condition. However, the vast majority of what Medicare and health insurance plans spend for patients with chronic conditions does not go to the physician practice that is managing the chronic condition, but to pharmaceutical companies for the drugs used to treat the chronic condition, to hospitals where the patients are treated for exacerbations of their condition, and to post-acute care providers following hospital stays.
FIGURE 32
Types of Avoidable Spending in Current Services for Patients with Chronic Conditions
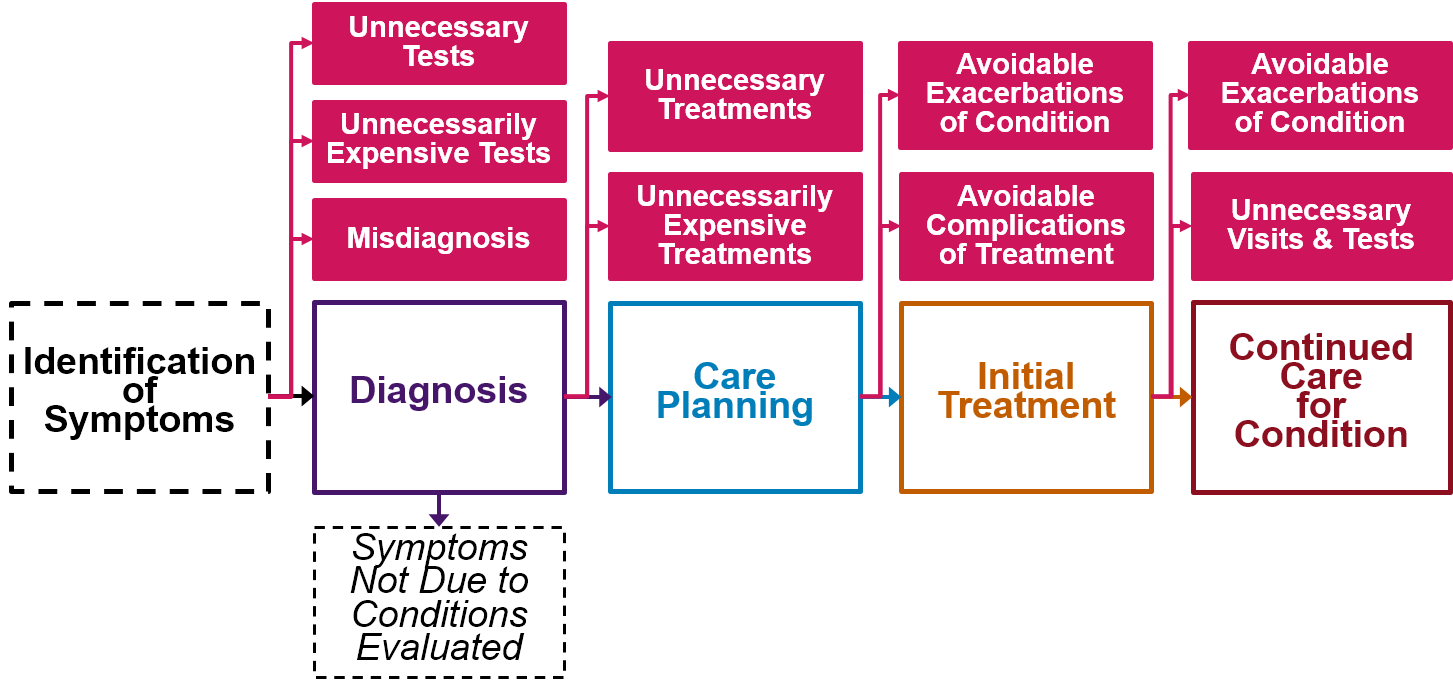
There is a significant amount of avoidable spending in other areas in each phase of care, as shown in Figure 32. This avoidable spending would likely decrease under Patient-Centered Payment because it would support:
- More accurate diagnosis. With an explicit focus on supporting accurate diagnosis, patients will be less likely to receive treatments for a disease they do not have and be more likely to receive effective treatments for the diseases they do have.
- Evidence-based treatment. With an explicit focus on developing written care plans consistent with evidence-based guidelines, patients will be less likely to receive unnecessary and unnecessarily-expensive medications and other treatments.
- Better prevention and management of exacerbations and complications of treatment. With better ability by physician practices to provide education to patients, to proactively monitor patients’ health, and to respond rapidly to problematic symptoms, patients will be less likely to experience disease exacerbations and less likely to need treatment for exacerbations in Emergency Departments and hospitals.
The reduction in avoidable spending has the potential to offset increases in spending on the services delivered by physician practices described in the previous section, resulting in a reduction in total spending for payers.
FIGURE 33
Impact of Patient-Centered Payment on Total Healthcare Spending
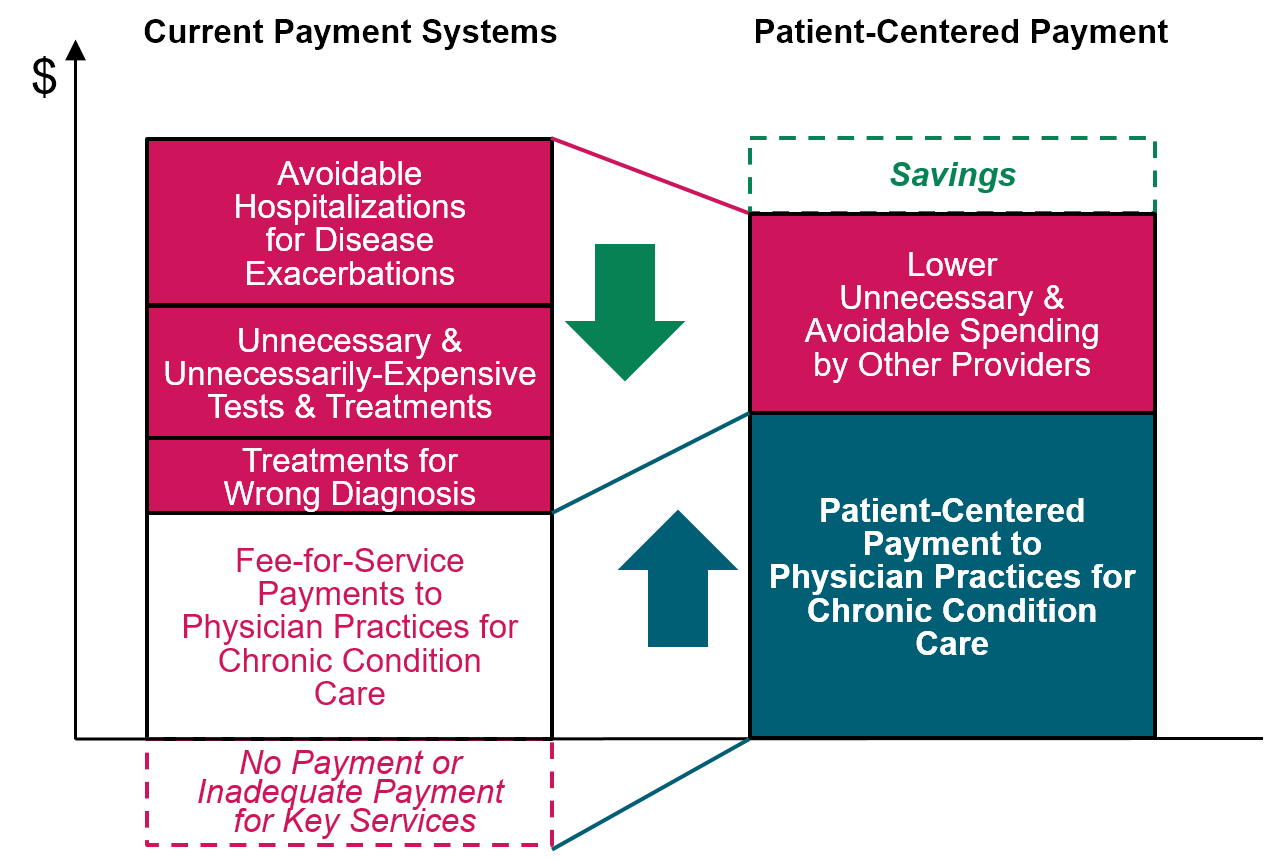
However, the fact that a reduction in total spending is likely does not mean that a physician practice’s eligibility to receive Patient-Centered Payment should be contingent on a decrease in total spending occurring. Total healthcare spending for patients with chronic conditions depends not only on the quality of the care they receive for the chronic condition, but also on the characteristics of the patients, the ways that other services (including services for other health problems) are delivered and paid for, and the cost-sharing requirements for services under their health insurance. For example,
For patients diagnosed with a chronic condition at an early stage, improved chronic condition care could cause an increase in total healthcare spending, because those individuals would be more likely to be prescribed and use medications and other treatments to successfully prevent the progression of the disease. Greater use of these services and medications is important for achieving lower spending and better health outcomes for the patients in the long run, but adequate payments to support current services to the patients can increase total healthcare spending in the short run.
If the prices of medications increase, or if the health insurance plan increases the amounts it pays for tests or procedures, then total spending on the patients’ care could increase even if patients receive fewer of those services.
If a specialist makes a more accurate diagnosis or develops a more cost-effective care plan, but the patient’s primary care practice does not provide appropriate condition management or the patient is unwilling to take appropriate actions to manage their condition, spending may increase for reasons beyond the control of the specialist.
Moreover, if total spending on a group of patients with chronic conditions does decrease, it does not necessarily mean that the patients are receiving better care; failure to deliver necessary services to a patient could reduce spending in the short term but result in higher spending in the future because the chronic condition could progress to a more severe stage more quickly. Payment models that make payments explicitly or implicitly contingent on whether there is a reduction in total healthcare spending, such as shared savings programs, can create perverse incentives to undertreat patients in ways that produce short-term savings but result in higher spending in the long run.
The right way to evaluate the effectiveness of a payment model is not based on whether spending decreases but whether the payments provide sufficient resources to cover the costs of delivering high-quality care to patients, and whether the accountability component ensures that every patient is receiving appropriate, high-quality care. Unfortunately, in the Medicare program, Congress required that the Center for Medicare and Medicaid Innovation (CMMI) focus on projects that will reduce total Medicare spending. Moreover, CMMI is prohibited from continuing or expanding a demonstration project unless the CMS Office of the Actuary certifies that total spending will not increase. As a practical matter, the Actuary will never certify a CMMI model unless an evaluation shows that it actually reduced total Medicare spending. Consequently, unless Congress changes the statute, it is unlikely that CMMI would ever implement a demonstration program using true Patient-Centered Payment.83
Impacts on Productivity and Employer Costs
Better care for patients with chronic conditions can also have a beneficial impact on worker productivity. Working-age individuals who have poorly managed chronic conditions are likely to either have absences from work or to have what is often called “presenteeism,” i.e., the individual is on the job but is not functioning efficiently or effectively. Analyses have estimated that for many types of common health problems, the cost of lost productivity from both absenteeism and presenteeism is much greater than the amount spent on healthcare services to treat them.84
Patient-Centered Payment for Care of Chronic Conditions can help physician practices improve worker productivity in several different ways:
- The physician practice can be organized to respond quickly when a patient has a new health problem or an exacerbation of an existing problem, rather than forcing a patient to suffer with symptoms for days or even weeks before being diagnosed and treated.
- The practice will have the flexibility and resources to provide services to patients in a way that is convenient for the patient’s work schedule and responsibilities. The patient will not be forced to miss work in order to come to the physician’s office for something that could have been addressed over the phone or through a telehealth visit, and the patient will not be forced to make multiple short visits to address what could be addressed in a single visit of adequate length.
- The practice will be accountable for delivering the evidence-based services to each patient that are most likely to successfully address their health problems, and the practice will have adequate time and staff to help patients understand and use those services.
- The practice will also be accountable for monitoring how well patients are doing so it can modify treatments (or the diagnosis) when the evidence-based services are not working well for a particular patient.
In addition, if a worker does not have a chronic disease, but they have a child who does, better management of the child’s condition will help the parent avoid missing work.
Higher worker productivity has a direct economic benefit for employers, both by reducing costs (e.g., avoiding the need to hire temporary workers) and increasing revenues (through the ability to deliver more products or services). The resulting higher profits experienced by the employer will offset at least some and potentially all of the higher amounts spent to support high-quality chronic condition care for its employees and their families. The employees also receive an economic benefit; hourly workers will have higher incomes if they miss fewer hours of work, and employees can be paid more if they increase the profitability of their employer.
The monetary benefits of higher productivity may well offset any net cost of higher payments for chronic condition care. However, the benefits of higher productivity accrue to the employer and employees, not to the employees’ health insurance plan. The cost of higher spending on physician services will be passed on directly to self-insured employers, but for small businesses and individuals that purchase health insurance directly, higher payments for these services will need to come out of the premiums collected by the health insurance companies. The benefits of improved productivity received by the small businesses and workers would help to offset any increase in insurance premiums they might need to pay to support higher payments to physician practices by the health insurance plan.
FIGURE 34
Impact of Patient-Centered Payment on Employer Costs
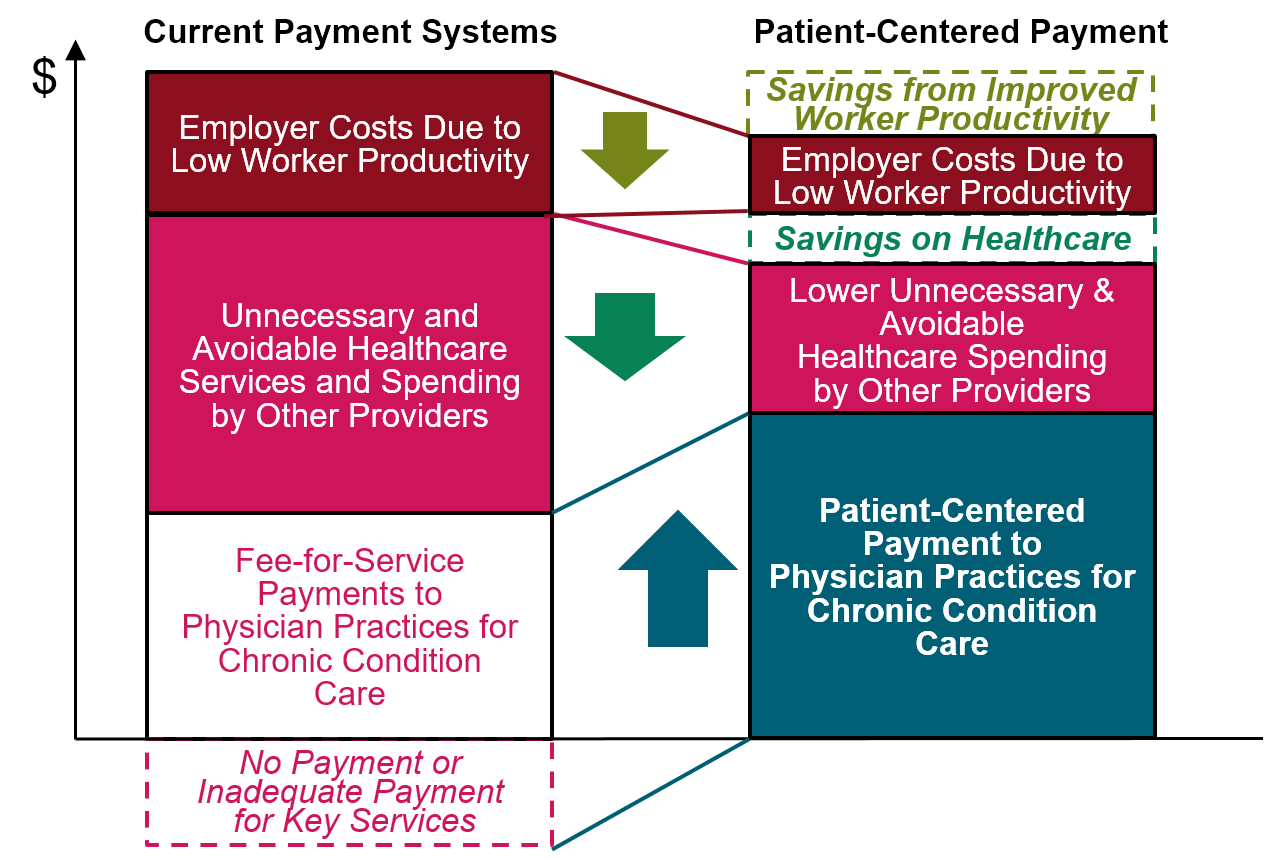
Implementing Patient-Centered Payment
Operationalizing Billing and Payment
Two actions will be needed in order to enable physician practices to bill for and receive Diagnosis Payments, Care Planning Payments, and Condition Management Payments:
- creating billing codes for each of the payment categories shown in Figure 24, and
- assigning adequate payment amounts to those billing codes.
Creation of Billing Codes and Rules
For patients who have insurance coverage, a physician practice is currently paid by submitting a claim form to the patient’s health insurance plan, with billing codes on the form describing the services delivered. Under Patient-Centered Payment, the appropriate codes for the new payments shown in Figure 24 (i.e., the Diagnosis Payment, the monthly Condition Management Payment, etc.) would be submitted on a claim form each month when the practice delivered the services associated with one or more of those payments to the patient during the month and did so in a way that was consistent with an evidence-based Clinical Practice Guideline.
Ideally, these codes should be part of the standard set of CPT (Current Procedural Terminology) codes that describe the services physicians deliver. To accomplish this, the American Medical Association’s CPT Editorial Panel would need to establish a formal definition for each of the patient-centered chronic condition care services (e.g., diagnosis of symptoms, care planning, or condition management) and assign a specific CPT code to that definition.
When the CPT Editorial Panel creates a new CPT code, it will also specify which other CPT codes should not be used for the same patient during the same period of time. These rules are then incorporated into the National Correct Coding Initiative (NCCI) Procedure-to-Procedure (PTP) Column One/Column Two Correct Coding edit file85 to ensure a claim containing the ineligible codes would not be paid.
Under Patient-Centered Payment for Care of Chronic Conditions, a practice that bills for services using the codes for Diagnosis Payments, Care Planning Payments, and Condition Management Payments should not also bill for services using existing Evaluation and Management Services CPT codes for Office or Other Outpatient Visits, for Principal Care Management Services, or for Chronic Care Management Services. However, the practice should be able to continue billing for other Evaluation and Management Services codes when appropriate; for example, the CPT codes for Initial Hospital Care and Subsequent Hospital Care would still be used if the physician is managing the care of a patient during a hospital stay.
Assigning Adequate Payment Amounts
It is not enough to create billing codes; if the amounts paid for the codes are not adequate, a physician practice will not be able to deliver high-quality care. Consequently, once the CPT codes for Patient-Centered Payment for Care of Chronic Conditions are defined, an adequate payment amount needs to be assigned to each code. The amount that Medicare and most health plans currently pay for a service delivered by a physician is determined through a two-step process: (1) the CPT code for the service is assigned a Relative Value Unit (RVU) amount and (2) each year, the RVU amount is multiplied by an annual Conversion Factor to determine the dollar amount of the payment.
Assigning RVUs to Payment Categories for Chronic Condition Care
RVUs for new billing codes are developed by the American Medical Association/Specialty Society RVS Update Committee, commonly known as the “RUC.” When the CPT Editorial Panel creates a new CPT code, the RUC develops a recommendation on the number of RVUs that should be assigned to that code. The RUC also reviews and makes adjustments to the RVU amounts for existing CPT codes when there is reason to believe they are no longer accurate.86 In most cases, the Centers for Medicare and Medicaid Services (CMS) uses the RVU values recommended by the RUC in determining Medicare payments, but it is not obligated to do so, and in some cases, it assigns a different number of RVUs to a CPT code than what the RUC has recommended.
Initially, it will be impossible for either the RUC or CMS to determine exactly what RVU amounts are “right” for the Patient-Centered Payment CPT codes. There is very little data on how much time and cost is involved in delivering high-quality care for chronic conditions because the current payment system prevents physician practices from delivering evidence-based services in the most effective way. The estimates in Section 3 can be used initially, but after the services are being delivered, the amounts will need to be revised based on information from physician practices about the actual time and costs required.
This is exactly the process that is currently used by the RUC to assign and update RVUs for all new CPT codes. When a new type of physician service is defined and a CPT code is assigned, the RUC engages in a process to estimate what the appropriate RVU amount for that service should be, using whatever data it can obtain and making informed assumptions in order to fill the gaps in data. After the service is being delivered, the RUC collects data on the actual time and costs involved and determines whether and how to revise the RVU value.
Determining an Appropriate Conversion Factor
As soon as estimates are made of the time and costs associated with delivering the services associated with the new CPT codes in order to assign the RVU amounts, the information on times and costs should also be translated into:
- an estimate of the optimal number of patients for whom a physician practice could provide high-quality chronic condition care;
- an estimate of the total number of RVUs for the new services the practice would deliver to those patients; and
- an estimate of the total amount of revenue that the practice would need to receive to cover its costs for the services delivered to those patients.
These estimates could be made using calculations similar to those shown in Section 3. The appropriate Conversion Factor can then be determined by dividing the estimated total revenue needed by the estimated total RVUs for the services that would be delivered.87
Although these types of calculations are not typically carried out by the RUC, the RVU values the RUC assigns will be of little benefit if they are not converted into adequate payment amounts. Consequently, it would be desirable if the RUC also recommended what the Conversion Factor should be in order to ensure payments are adequate.
Each year, the Conversion Factor will need to be updated based on inflation, and the RVUs and Conversion Factor should be periodically re-evaluated to ensure they reflect the current costs of delivering evidence-based services
Setting an Appropriate Conversion Factor for Medicare Payments
In the Medicare program, the Centers for Medicare and Medicaid Services (CMS) establishes a new conversion factor each year through regulation, using a methodology specified in statute. The Medicare conversion factor was originally supposed to be increased every year by an Update Factor designed to reflect inflation (as measured by the Medicare Economic Index). However, Congress now specifies the annual Update Factor in law, and it is no longer based on actual inflation amounts.88 Unfortunately, this has caused the actual payments to physician practices for most services to be inappropriately low. As a result of both the low annual updates and budget neutrality requirements, the Medicare Conversion Factor in 2021 was almost 9% lower than it was two decades earlier in 2001, even though the amounts that physician practices have to pay for staff, insurance, supplies, and office space increased during that time.
Because of this, the Conversion Factor that is needed to ensure adequate amounts for Patient-Centered Payment in Medicare is likely to be significantly higher than the standard Conversion Factor used by CMS. Consequently, for physician practices participating in Patient-Centered Payment, CMS will need to make an adjustment to the payment amounts that would be determined using its standard Conversion Factor. CMS already makes a number of “policy adjustments” to payment amounts after multiplying RVUs by the standard Conversion Factor, including reductions for non-participating physicians, bonuses for physicians practicing in Health Professional Shortage Areas, and increases or decreases specified under the Quality Payment Program based on performance in the Merit-Based Incentive Payment System and participation in Alternative Payment Models. Adjustments to ensure adequate amounts for Patient-Centered Payment could be made through a similar process.
Setting an Appropriate Conversion Factor for Health Insurance Plan Payments
Health insurance plans are not required to use the Medicare Conversion Factor and they frequently use different conversion factors for different physician practices. If the Conversion Factor needed to create adequate amounts for Patient-Centered Payment is higher than what the plan is currently using to pay a physician practice, the health plan would need to make an adjustment to that plan’s Conversion Factor, similar to what is described for Medicare. Some payers pay for services using fee schedules that bear no relation to the RVU structure. These payers would need to establish amounts for each payment category in Patient-Centered Payment based on the results of the analysis of costs described above.
Making Patient-Centered Payment Available to Physician Practices
It does little good to define the CPT codes, appropriate RVU amounts, and adequate Conversion Factor necessary for implementation of Patient-Centered Payment for Care of Chronic Conditions if health insurance plans, Medicare, and Medicaid programs are not willing to use them to pay physician practices. Moreover, it will be difficult to justify doing the work needed to carry out these preparatory steps properly if there is little or no confidence that the work will actually be used by payers to improve the way physician practices are paid.
Every person who has a chronic condition should have the ability to receive high-quality care for that condition regardless of what type of insurance they have. Consequently, every payer – every commercial insurance plan, every Medicare Advantage plan, every Medicaid Managed Care Organization, every state Medicaid agency, and Original (fee-for-service) Medicare – should agree to make Patient-Centered Payment for Care of Chronic Conditions available to any physician practice providing services to the patients insured by that payer so that all patients with a chronic condition have the opportunity to receive high-quality care.
Making Patient-Centered Payment available to all physician practices does not mean that a payer should require that every practice be paid in this way. Some practices may not be willing or able to immediately change the way they deliver care consistent with the expectations of Patient-Centered Payment for Care of Chronic Conditions. There is no need to hold back the practices that are willing to change, or to delay payments for practices that are already delivering high-quality care and losing money doing so. Most physician practices that manage the care of patients with chronic conditions want a better payment system than they have today, and most practices will likely want to participate once they see that a payer is implementing Patient-Centered Payment properly.
Moreover, once patients with chronic conditions see how much better care can be under a better payment system, they will want to receive the kind of care that practices can deliver when they participate in the Patient-Centered Payment system. As long as patients have a choice of which physician practices to use, the patients can switch to a practice that delivers patient-centered care, which will help to encourage practices to begin using Patient-Centered Payment for Care of Chronic Conditions. In addition, if patients have a choice of insurance plans, they can choose a plan which will pay their physicians using Patient-Centered Payment.
Footnotes
Boersma P, Black LI, Ward BW. “Prevalence of Multiple Chronic Conditions Among US Adults, 2018.” Preventing Chronic Disease 17:E106 (2020).↩︎
Rezaee ME, Pollock M. “Multiple Chronic Conditions Among Outpatient Pediatric Patients, Southeastern Michigan, 2008–2013.” Preventing Chronic Disease 12:E18 (2015).↩︎
Buttorf C, Ruder T, Bauman M. Multiple Chronic Conditions in the United States. RAND Corporation (2017).↩︎
Ready, Risk, Reward: Improving Care for Patients with Chronic Conditions. Premier, Inc. (2019).
Gregg EW, Hora I, Benoit SR. “Resurgence in Diabetes-Related Complications.” JAMA 321(19):1867-1868 (2019).↩︎Goetzel RZ et al. “Health, Absence, Disability, and Presenteeism Cost Estimates of Certain Physical and Medical Conditions Affecting U.S. Employers.” Journal of Occupational and Environmental Medicine 46(4):398-412 (2004).↩︎
Miller HD. Patient-Centered Payment for Primary Care. Center for Healthcare Quality and Payment Reform (2021).↩︎
Committee on Diagnostic Error in Health Care. Improving Diagnosis in Health Care. The National Academies Press (2015).↩︎
Mitchell DM. “The Critical Role of Hospitalists in Controlling Healthcare Costs,” Journal of Hospital Medicine 5(3):127-132 (2010).↩︎
Lipska KJ, Krumholz HM. “Is Hemoglobin A1C the Right Outcome for Studies of Diabetes?” JAMA 317(10):1017-1018 (2017).↩︎
Center for Medicare and Medicaid Innovation. Bundled Payments for Care Improvement (BPCI) Initiative.↩︎
Center for Medicare and Medicaid Innovation. BPCI Advanced.↩︎
McWilliams JM. “Cost Containment and the Tale of Care Coordination,” New England Journal of Medicine 375(23): 2218-2220 (2016).↩︎
Center for Medicare and Medicaid Innovation. Global and Professional Direct Contracting Model.↩︎
In addition, services from different specialists might be needed in different phases, e.g., if the specialist who initially diagnoses the patient determines that the patient should be treated by a different physician who subspecializes in treating the specific condition subtype for that patient.↩︎
Prior to 2021, there were additional requirements for billing E/M codes that were even more problematic for specialists with good diagnostic skills. Under those rules, a specialist who could immediately determine what was causing a patient’s symptoms in a brief visit could not be paid at all if they did not complete a patient history and perform an examination.↩︎
American Medical Association. CPT E/M Office Revisions Level of Medical Decision Making (MDM).↩︎
Miller HD. Patient-Centered Payment for Primary Care. Center for Healthcare Quality and Payment Reform (2021).↩︎
Singh D et al. “Use of Rheumatologic Testing in Patients Who Eventually Receive a Diagnosis of Rheumatoid Arthritis,” Southern Medical Journal 112(10): 535-538 (2019).↩︎
Although there are currently several billing codes that can be used to pay specialists for consultative services (CPT codes 99446-99449 and 99451), they require that the specialist provide a written report to the primary care physician (PCP) on the specific patient being evaluated, which would require more time than simply providing advice and support for the PCP about how to evaluate specific kinds of symptoms for the patient.↩︎
If there are certain tests that are always needed for a particular type of diagnosis and if those tests are typically performed by the physician practice itself rather than by an outside laboratory, then the payment for those tests could be “bundled” into the Diagnosis Payment for that type of patient and practice. The purpose of this would be to simplify billing for the practice and create a more predictable payment for the patient. However, this would require creation of an additional billing code that is specifically targeted to that type of diagnosis and that would be assigned a higher payment amount to reflect the fact that testing costs would also be included.↩︎
Sox HC, Stewart WF. “Algorithms, Clinical Practice Guidelines, and Standardized Clinical Assessment and Management Plans: Evidence-Based Patient Management Standards in Evolution.” Academic Medicine 90(2) (2015).↩︎
National Asthma Education and Prevention Program Coordinating Committee Expert Panel Working Group. 2020 Focused Updates to the Asthma Management Guidelines. National Heart, Lung, and Blood Institute, National Institutes of Health, U.S Department of Health and Human Services (December 2020).
National Asthma Education and Prevention Program. Guidelines for the Diagnosis and Management of Asthma. National Heart, Lung, and Blood Institute, National Institutes of Health, U.S Department of Health and Human Services (August 2007).↩︎Global Initiative for Chronic Obstructive Lung Disease. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease – 2021 Report.↩︎
American Diabetes Association. “Standards of Medical Care in Diabetes – 2018.” Diabetes Care 41 (Supplement 1) January 2018.↩︎
Garber AJ et al. “Consensus Statement by the American Association of Clinical Endocrinologists and American College of Endocrinology on the Comprehensive Type 2 Diabetes Management Algorithm.” Endocrine Practice 24(1): 91-120 (2018).↩︎
Yancy CW et al. “2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure.” Journal of the American College of Cardiology 70(6): 776-803 (2017).
Yancy CW, et al. “2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines.” Circulation 128:e240-e327 (2013).↩︎Fihn SD, Blankenship JC et al. “Focused Update of the Guideline for the Diagnosis and Management of Patients With Stable Ischemic Heart Disease.” Journal of the American College of Cardiology 64(18): 1929-1949 (2014).
Fihn SD, Gardin JM et al. “2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS Guideline for the Diagnosis and Management of Patients With Stable Ischemic Heart Disease.” Journal of the American College of Cardiology 60(24): e44-e164 (2012).↩︎Kuntz G. “What Do We Mean When We Talk About ‘Clinical Pathways?’” Journal of Clinical Pathways (January/February 2019).↩︎
Farias M et al. “Provider Attitudes Toward Standardized Clinical Assessment and Management Plans (SCAMPs).” Congenital Heart Disease 6(6) (2011).↩︎
Spencer-Bonilla G, Quiñones AR, Montori VM. “Assessing the Burden of Treatment.” Journal of General Internal Medicine 32(10:1141-1145 (2017).↩︎
Carlsen B, Glenton C, Pope C. “Thou Shalt Versus Thou Shalt Not: A Meta-Synthesis of GPs’ Attitudes To Clinical Practice Guidelines.” British Journal of General Practice 57:971-978 (2007).↩︎
Farias M et al. “Standardized Clinical Assessment and Management Plans (SCAMPs) Provide A Better Alternative to Clinical Practice Guidelines.” Health Affairs 32(5) (2013).↩︎
Kuhlman J et al. “Clinical Transformation Through Change Management Case Study: Chest Pain in the Emergency Department.” EClinical Medicine 10 (2019).↩︎
Committee on Diagnostic Error in Health Care. Improving Diagnosis in Health Care. The National Academies Press (2015).↩︎
The Medical Group Management Association reports benchmarking data for physician practices in terms of costs per full-time-equivalent physician, and most analyses of the costs of delivering physician services report their findings in the same way, which implicitly assumes that costs are proportional to the number of physicians.↩︎
Pope GC, Burge RT. “Economies of Scale in Physician Practice.” Medical Care Research and Review 53(4):417-440 (1996).
Burns LR, Goldsmith JC, Sen A. “Horizontal and Vertical Integration of Physicians: A Tale of Two Tails”, Annual Review of Health Care Management: Revisiting the Evolution of Health Systems Organization Advances in Health Care Management, Vol. 15, pp. 39-117 (2014).↩︎Kane L. Medscape Physician Compensation Report 2021. Medscape, April 16, 2021.↩︎
U.S. Department of Labor, Bureau of Labor Statistics. May 2020 National Occupational Employment and Wage Estimates, United States.↩︎
The benefits for the physician are assumed to cost $30,000 per year, and benefits for other staff are assumed to cost an amount equal to 20% of their salary.↩︎
American Medical Association. CPT E/M Office Revisions Level of Medical Decision Making (MDM).↩︎
Although there are currently several billing codes that can be used to pay specialists for consultative services (CPT codes 99446-99449 and 99451), they require that the specialist provide a written report to the primary care physician on the specific patient being evaluated, which would require more time than simply providing advice and support for the PCP about how to design a care plan for the patient.↩︎
Sox HC, Stewart WF. “Algorithms, Clinical Practice Guidelines, and Standardized Clinical Assessment and Management Plans: Evidence-Based Patient Management Standards in Evolution.” Academic Medicine 90(2) (2015).↩︎
Kuntz G. “What Do We Mean When We Talk About ‘Clinical Pathways?’” Journal of Clinical Pathways January/February 2019.↩︎
Farias M et al. “Provider Attitudes Toward Standardized Clinical Assessment and Management Plans (SCAMPs).” Congenital Heart Disease 6(6) (2011).↩︎
Spencer-Bonilla G, Quiñones AR, Montori VM. “Assessing the Burden of Treatment.” Journal of General Internal Medicine 32(10:1141-1145 (2017).↩︎
Carlsen B, Glenton C, Pope C. “Thou Shalt Versus Thou Shalt Not: A Meta-Synthesis of GPs’ Attitudes To Clinical Practice Guidelines.” British Journal of General Practice 57:971-978 (2007).↩︎
Spatz ES, Krumholz HM, Moulton BW. “Prime Time for Shared Decision Making,” JAMA 317(13):1309-1310 (2017).↩︎
National Asthma Education and Prevention Program. Guidelines for the Diagnosis and Management of Asthma. National Heart, Lung, and Blood Institute, National Institutes of Health, U.S Department of Health and Human Services (August 2007).↩︎
U.S. Department of Labor, Bureau of Labor Statistics. May 2020 National Occupational Employment and Wage Estimates, United States.↩︎
The benefits for the nurse are assumed to cost an amount equal to 20% of the salary.↩︎
Attribution systems assign patients to a physician practice based on whether the patient made more office visits to that practice than to other practices. This approach is problematic for many reasons. For example, if a physician practice helps a patient successfully manage their chronic condition without making office visits to the practice, the patient may not be attributed to the practice, thereby preventing the practice from receiving a monthly payment to support that work.↩︎
For example, the use of corticosteroids in treating patients with severe asthma or COPD can increase blood sugar levels and make it more difficult to treat diabetes if the patient is also diabetic.↩︎
Resneck JS. “Refocusing Medication Prior Authorization on Its Intended Purpose.” JAMA 323(8):703-704 (2020).↩︎
Casalino LP et al. “What Does It Cost Physician Practices to Interact With Health Insurance Plans?” Health Affairs 28(4):w533-w543 (2009).↩︎
Wasson JH. “Standardized Assessment, Information, and Networking Technologies (SAINTs): Lessons From Three Decades of Development and Testing.” Quality of Life Research (2020).↩︎
Ibid .↩︎
Ho L, Antonucci J. “Using Patient-Entered Data to Supercharge Self-Management.” Annals of Family Medicine 15(4):382 (2017).↩︎
Wasson JH et al. “Development of a Care Guidance Index Based on What Matters to Patients.” Quality of Life Research 27:51-58 (2018).↩︎
Wasson JH, Ho L, Soloway L, Moore LG. “Validation of the What Matters Index: A brief, patient-reported index that guides care for chronic conditions and can substitute for computer-generated risk models.” PLoS ONE 13(2): e0192475.↩︎
Wasson JH et al. “Patients Use the Internet to Enter the Medical Home.” Journal of Ambulatory Care Management 34(1):38-46 (2011).↩︎
Ho L et al. “The Right Tool for the Right Job: The Value of Alternative Patient Experience Measures.” Journal of Ambulatory Care Management 36(3):241-244 (2013).↩︎
Kupfer JM, Bond EU. “Patient Satisfaction and Patient-Centered Care: Necessary But Not Equal.” JAMA 308(2):139-140 (2012).↩︎
For example, the Primary Care First demonstration program in Medicare increases payments to a primary care practice by up to 50% or reduces them by up to 10% based primarily on the overall rate of hospitalizations for patients in the practice. Center for Medicare and Medicaid Innovation. Primary Care First: Payment and Attribution Methodologies PY2022 (2021).↩︎
Farias M et al. “Standardized Clinical Assessment and Management Plans (SCAMPs) Provide A Better Alternative to Clinical Practice Guidelines.” Health Affairs 32(5) (2013).↩︎
Østbye T et al. “Is There Time for Management of Patients With Chronic Diseases in Primary Care?” Annals of Family Medicine 3(3): 209-214 (2005).↩︎
The study assumed the types of chronic conditions were similar to the prevalence in the U.S. population, and that some patients had uncontrolled conditions whereas others had well-controlled conditions.↩︎
Current national data indicate that more than half (52%) of U.S. adults have one or more chronic conditions. Boersma P, Black LI, Ward BW. “Prevalence of Multiple Chronic Conditions Among US Adults, 2018,” Preventing Chronic Disease 17:E106 (2020). The analysis by Østbye et al. assumed that 25% of the patients in the practice were under age 18; estimates of the percentage of children and adolescents with chronic conditions range from 16% to 40%, but all estimates indicate the rate is lower than the rate for adults. As a result, the rate for the total patient panel would likely be between 40% and 50%. Moreover, the study was conducted using data from 2001 and 2002, and the prevalence of chronic disease was likely lower then than what is reported in more recent data.↩︎
Altschuler J et al. “Estimating a Reasonable Patient Panel Size for Primary Care Physicians With Team-Based Task Delegation.” Annals of Family Medicine 10(5): 396-400 (2012).↩︎
Huynh P, Toulouse A, Hirsch I. “One-Year Time Analysis in an Academic Diabetes Clinic: Quantifying Our Burden.” Endocrine Practice 24(5):489-491 (May 2018).↩︎
Centers for Medicare and Medicaid Services. Physician Fee Schedule.↩︎
Centers for Medicare and Medicaid Services. “Medicare Program; CY 2022 Payment Policies Under the Physician Fee Schedule and Other Changes to Part B Payment Policies,” Federal Register 86 (221): 65274-65275 (November 19, 2021).↩︎
Centers for Medicare and Medicaid Services. “Medicare Program; CY 2022 Payment Policies Under the Physician Fee Schedule and Other Changes to Part B Payment Policies,” Federal Register 86 (221): 65117-65118 (November 19, 2021).↩︎
Ibid .↩︎
The patients receiving services supported by the Principal Care Management payments could have more than one chronic condition, but the payments are intended to support management of only one chronic condition, and a different physician practice could receive a similar payment if its staff spend at least 30 minutes of time during the month managing a different chronic condition.↩︎
Centers for Medicare and Medicaid Services. “Medicare Program; Revisions to Payment Policies Under the Physician Fee Schedule, Clinical Laboratory Fee Schedule & Other Revisions to Part B for CY 2014.” Federal Register 78 (139): 43340 (July 19, 2013).↩︎
Centers for Medicare and Medicaid Services. “Medicare Program; Revisions to Payment Policies Under the Physician Fee Schedule, Clinical Laboratory Fee Schedule & Other Revisions to Part B for CY 2014.” Federal Register 78 (237): 74414-74427 (December 10, 2013).↩︎
The expected hospitalization rates would have to be estimated for the complex patient and treatment regimen categories using information available in claims data.↩︎
In the Medicare program, the statutory amount is ASP + 6%, but under Congressional sequestration requirements, the actual amount is ASP + 4.3%. Many commercial insurance companies pay a higher percentage above ASP than Medicare does.↩︎
Additional details on the problems with the current ASP+x% methodology are available in Miller HD. A Better Way to Pay for Cancer Care. Center for Healthcare Quality and Payment Reform (2019).↩︎
Alternatively, the practice would need to enroll even more patients and hire additional physicians and other staff.↩︎
Miller HD. How to Create More Successful Alternative Payment Models in Medicare. Center for Healthcare Quality and Payment Reform (2020).↩︎
Goetzel RZ et al. “Health, Absence, Disability, and Presenteeism Cost Estimates of Certain Physical and Medical Conditions Affecting U.S. Employers.” Journal of Occupational and Environmental Medicine 46(4):398-412 (2004).
Loeppke R et al. “Health and Productivity as a Business Strategy: A Multiemployer Study.” Journal of Occupational and Environmental Medicine 51(4): 411-428 (2009).↩︎The PTP Column One/Column Two Correct Coding edit file is available here↩︎
American Medical Association. RVS Update Process. (2022).↩︎
Since the actual total revenue would be the sum of the RVUs times the Conversion Factor, the appropriate Conversion Factor would be equal to the total revenue needed divided by the sum of the RVUs for the services delivered.↩︎
Prior to 2015, Congress required that the update based on the Medicare Economic Index be modified by the “Sustainable Growth Rate” (SGR) formula. This formula threated large cuts in physician fees every year. In 2015, as part of the Medicare Access and CHIP Reauthorization Act (MACRA), Congress repealed the SGR, but it also eliminated any connection between the Update Factors and inflation.↩︎